

Leveraging Linkage of Cohort Studies With Administrative Claims Data to Identify Individuals With Cancer
- PMID: 29334524
- PMCID: PMC6043405
- DOI: 10.1097/MLR.0000000000000875
Leveraging Linkage of Cohort Studies With Administrative Claims Data to Identify Individuals With Cancer
Abstract
Background: In an effort to overcome quality and cost constraints inherent in population-based research, diverse data sources are increasingly being combined. In this paper, we describe the performance of a Medicare claims-based incident cancer identification algorithm in comparison with observational cohort data from the Nurses' Health Study (NHS).
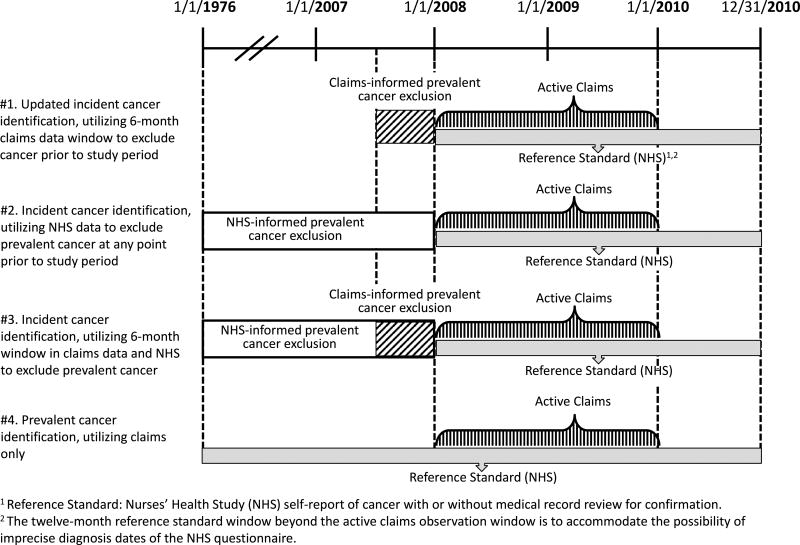
Methods: NHS-Medicare linked participants' claims data were analyzed using 4 versions of a cancer identification algorithm across 3 cancer sites (breast, colorectal, and lung). The algorithms evaluated included an update of the original Setoguchi algorithm, and 3 other versions that differed in the data used for prevalent cancer exclusions.
Results: The algorithm that yielded the highest positive predictive value (PPV) (0.52-0.82) and κ statistic (0.62-0.87) in identifying incident cancer cases utilized both Medicare claims and observational cohort data (NHS) to remove prevalent cases. The algorithm that only used NHS data to inform the removal of prevalent cancer cases performed nearly equivalently in statistical performance (PPV, 0.50-0.79; κ, 0.61-0.85), whereas the version that used only claims to inform the removal of prevalent cancer cases performed substantially worse (PPV, 0.42-0.60; κ, 0.54-0.70), in comparison with the dual data source-informed algorithm.
Conclusions: Our findings suggest claims-based algorithms identify incident cancer with variable reliability when measured against an observational cohort study reference standard. Self-reported baseline information available in cohort studies is more effective in removing prevalent cancer cases than are claims data algorithms. Use of claims-based algorithms should be tailored to the research question at hand and the nature of available observational cohort data.
Figures
Similar articles
-
An algorithm for the use of Medicare claims data to identify women with incident breast cancer.Health Serv Res. 2004 Dec;39(6 Pt 1):1733-49. doi: 10.1111/j.1475-6773.2004.00315.x. Health Serv Res. 2004. PMID: 15533184 Free PMC article.
-
Validation of a Medicare Claims-based Algorithm for Identifying Breast Cancers Detected at Screening Mammography.Med Care. 2016 Mar;54(3):e15-22. doi: 10.1097/MLR.0b013e3182a303d7. Med Care. 2016. PMID: 23929404 Free PMC article.
-
Evaluation of three algorithms to identify incident breast cancer in Medicare claims data.Health Serv Res. 2007 Oct;42(5):2056-69. doi: 10.1111/j.1475-6773.2007.00705.x. Health Serv Res. 2007. PMID: 17850533 Free PMC article.
-
Development and Validation of Claims-Based Definitions to Identify Incident and Prevalent Inflammatory Bowel Disease in Administrative Healthcare Databases.Inflamm Bowel Dis. 2023 Dec 5;29(12):1993-1996. doi: 10.1093/ibd/izad053. Inflamm Bowel Dis. 2023. PMID: 37043675 Free PMC article. Review.
-
Measuring abortion in claims data: What is the state of the science?Contraception. 2025 Feb;142:110750. doi: 10.1016/j.contraception.2024.110750. Epub 2024 Nov 15. Contraception. 2025. PMID: 39551368 Free PMC article. Review.
Cited by
-
Association of Breast Cancer Screening Behaviors With Stage at Breast Cancer Diagnosis and Potential for Additive Multi-Cancer Detection via Liquid Biopsy Screening: A Claims-Based Study.Front Oncol. 2021 Jun 15;11:688455. doi: 10.3389/fonc.2021.688455. eCollection 2021. Front Oncol. 2021. PMID: 34222015 Free PMC article.
-
Serious Illness and End-of-Life Treatments for Nurses Compared with the General Population.J Am Geriatr Soc. 2019 Aug;67(8):1582-1589. doi: 10.1111/jgs.16044. Epub 2019 Jul 9. J Am Geriatr Soc. 2019. PMID: 31287929 Free PMC article.
-
Antidepressant Use Trajectories and Risk of Discontinuation After Adolescents and Young Adult Cancer Diagnosis.Pharmacoepidemiol Drug Saf. 2025 Apr;34(4):e70131. doi: 10.1002/pds.70131. Pharmacoepidemiol Drug Saf. 2025. PMID: 40130769 Free PMC article.
-
Association of rurality, socioeconomic status, and race with pancreatic cancer surgical treatment and survival.J Natl Cancer Inst. 2023 Oct 9;115(10):1171-1178. doi: 10.1093/jnci/djad102. J Natl Cancer Inst. 2023. PMID: 37233399 Free PMC article.
-
Surgeon and Care Team Network Measures and Timely Breast Cancer Treatment.JAMA Netw Open. 2024 Aug 1;7(8):e2427451. doi: 10.1001/jamanetworkopen.2024.27451. JAMA Netw Open. 2024. PMID: 39207756 Free PMC article.
References
-
- Setoguchi S, Solomon DH, Glynn RJ, et al. Agreement of diagnosis and its date for hematologic malignancies and solid tumors between Medicare claims and cancer registry data. Cancer Causes Control. 2007;18(5):561–9. - PubMed
-
- Baldi I, Vicari P, Di Cuonzo D, et al. A high positive predictive value algorithm using hospital administrative data identified incident cancer cases. J Clin Epidemiol. 2008;61(4):373–9. - PubMed
-
- Couris CM, Polazzi S, Olive F, et al. Breast cancer incidence using administrative data: correction with sensitivity and specificity. J Clin Epidemiol. 2009;62(6):660–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
