

Thoracic aortic aneurysm in patients with loss of function Filamin A mutations: Clinical characterization, genetics, and recommendations
- PMID: 29334594
- PMCID: PMC7534149
- DOI: 10.1002/ajmg.a.38580
Thoracic aortic aneurysm in patients with loss of function Filamin A mutations: Clinical characterization, genetics, and recommendations
Abstract
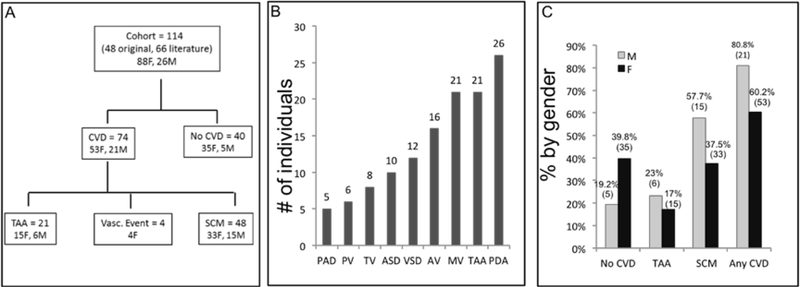
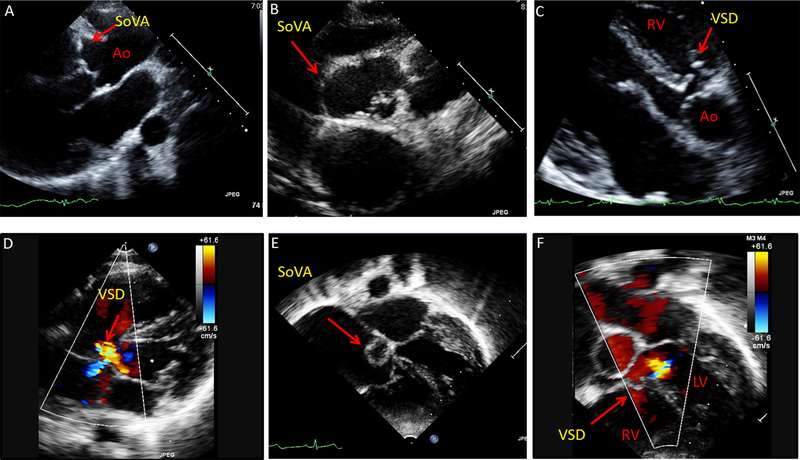
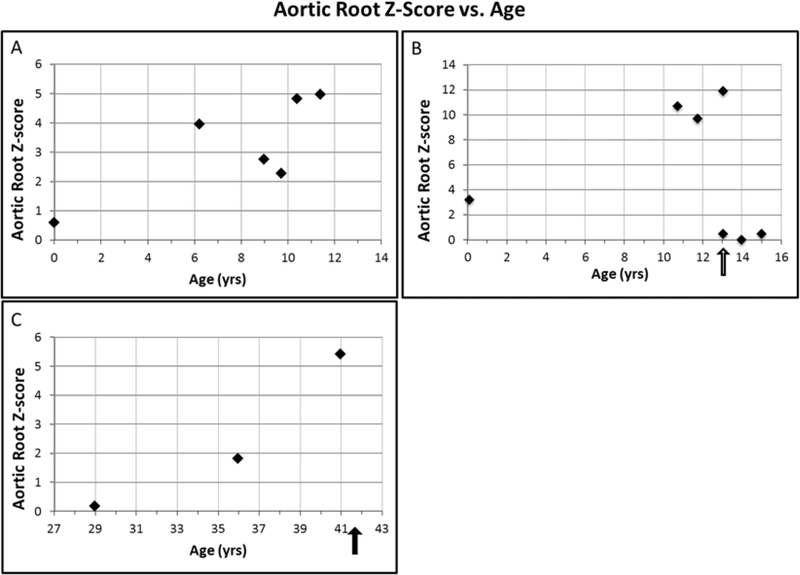
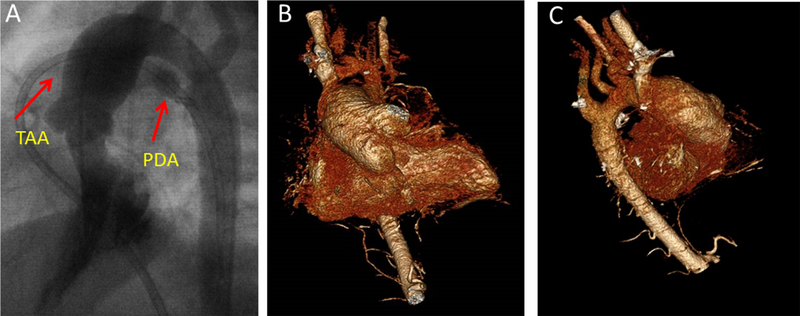
The frequency and gender distribution of thoracic aortic aneurysm as a cardiovascular manifestation of loss-of-function (LOF) X-linked FilaminA (FLNA) mutations are not known. Furthermore, there is very limited cardiovascular morbidity or mortality data in children and adults. We analyzed cardiac data on the largest series of 114 patients with LOF FLNA mutations, both children and adults, with periventricular nodular heterotopia (PVNH), including 48 study patients and 66 literature patients, median age of 22.0 years (88 F, 26 M, range: 0-71 years), with 75 FLNA mutations observed in 80 families. Most (64.9%) subjects had a cardiac anomaly or vascular abnormality (80.8% of males and 60.2% of females). Thoracic aortic aneurysms or dilatation (TAA) were found in 18.4% (n = 21), and were associated with other structural cardiac malformations in 57.1% of patients, most commonly patent ductus arteriosus (PDA) and valvular abnormalities. TAA most frequently involved the aortic root and ascending aorta, and sinus of Valsalva aneurysms were present in one third of TAA patients. Six TAA patients (28.5%) required surgery (median age 37 yrs, range 13-41 yrs). TAA with its associated complications was also the only recorded cause of premature, non-accidental mortality in adults (2 M, 2 F). Two adult patients (1 F, 1 M, median 38.5 yrs), died of spontaneous aortic rupture at aortic dimensions smaller than current recommendations for surgery for other aortopathies. Data from this largest series of LOF FLNA mutation patients underscore the importance of serial follow-up to identify and manage these potentially devastating cardiovascular complications.
Keywords: anomalies; aortic aneurysm; cardiac; filaminA; patent ductus arteriosus; periventricular nodular heterotopia; thoracic.
© 2018 Wiley Periodicals, Inc.
Figures

References
-
- Chen MH, & Walsh CA (2015). FLNA-Related Periventricular Nodular Heterotopia. In Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, & Stephens K (Eds.), GeneReviews(R) Seattle (WA).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
