

Periodontal Disease, Regular Dental Care Use, and Incident Ischemic Stroke
- PMID: 29335336
- PMCID: PMC5780242
- DOI: 10.1161/STROKEAHA.117.018990
Periodontal Disease, Regular Dental Care Use, and Incident Ischemic Stroke
Abstract
Background and purpose: Periodontal disease is independently associated with cardiovascular disease. Identification of periodontal disease as a risk factor for incident ischemic stroke raises the possibility that regular dental care utilization may reduce the stroke risk.
Methods: In the ARIC (Atherosclerosis Risk in Communities) study, pattern of dental visits were classified as regular or episodic dental care users. In the ancillary dental ARIC study, selected subjects from ARIC underwent fullmouth periodontal measurements collected at 6 sites per tooth and classified into 7 periodontal profile classes (PPCs).
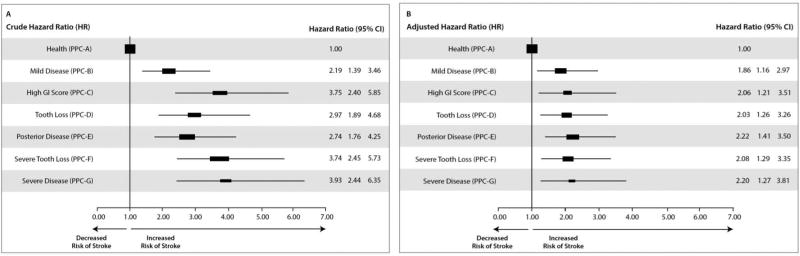
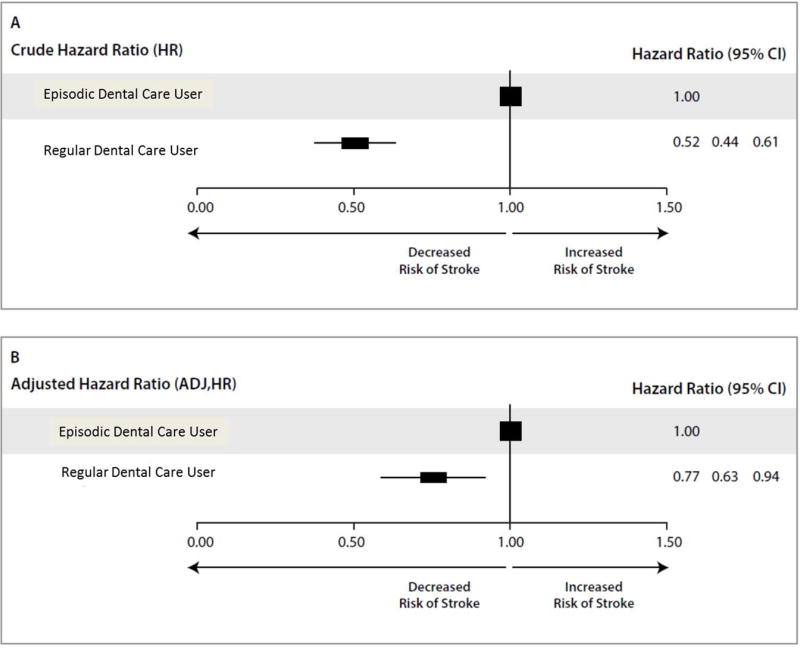
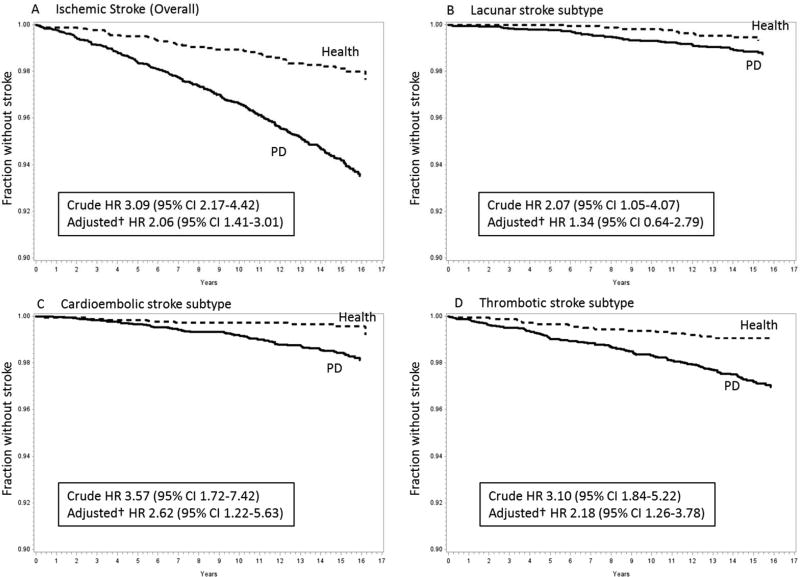
Results: In the ARIC study 10 362 stroke-free participants, 584 participants had incident ischemic strokes over a 15-year period. In the dental ARIC study, 6736 dentate subjects were assessed for periodontal disease status using PPC with a total of 299 incident ischemic strokes over the 15-year period. The 7 levels of PPC showed a trend toward an increased stroke risk (χ2 trend P<0.0001); the incidence rate for ischemic stroke/1000-person years was 1.29 for PPC-A (health), 2.82 for PPC-B, 4.80 for PPC-C, 3.81 for PPC-D, 3.50 for PPC-E, 4.78 for PPC-F, and 5.03 for PPC-G (severe periodontal disease). Periodontal disease was significantly associated with cardioembolic (hazard ratio, 2.6; 95% confidence interval, 1.2-5.6) and thrombotic (hazard ratio, 2.2; 95% confidence interval, 1.3-3.8) stroke subtypes. Regular dental care utilization was associated with lower adjusted stroke risk (hazard ratio, 0.77; 95% confidence interval, 0.63-0.94).
Conclusions: We confirm an independent association between periodontal disease and incident stroke risk, particularly cardioembolic and thrombotic stroke subtype. Further, we report that regular dental care utilization may lower this risk for stroke.
Keywords: atherosclerosis; dental care; gingivitis; risk factors; stroke.
© 2018 American Heart Association, Inc.
Figures
References
-
- Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005;366:1809–1820. - PubMed
-
- Eke PI, Jaramillo F, Thornton-Evans GO, Borgnakke WS. Dental visits among adult Hispanics--BRFSS 1999 and 2006. J Public Health Dent. 2011;71:252–256. - PubMed
-
- Mustapha IZ, Debrey S, Oladubu M, Ugarte R. Markers of systemic bacterial exposure in periodontal disease and cardiovascular disease risk: a systematic review and meta-analysis. J Periodontol. 2007;78:2289–2302. - PubMed
-
- Romagna C, Dufour L, Troisgros O, Lorgis L, Richard C, Buet P, et al. Periodontal disease: a new factor associated with the presence of multiple complex coronary lesions. J Clin Periodontol. 2012;39:38–44. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- R01 MD009738/MD/NIMHD NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- K23 DE025093/DE/NIDCR NIH HHS/United States
- R01 DE011551/DE/NIDCR NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
