

RFA Guardian: Comprehensive Simulation of Radiofrequency Ablation Treatment of Liver Tumors
- PMID: 29335429
- PMCID: PMC5768804
- DOI: 10.1038/s41598-017-18899-2
RFA Guardian: Comprehensive Simulation of Radiofrequency Ablation Treatment of Liver Tumors
Abstract
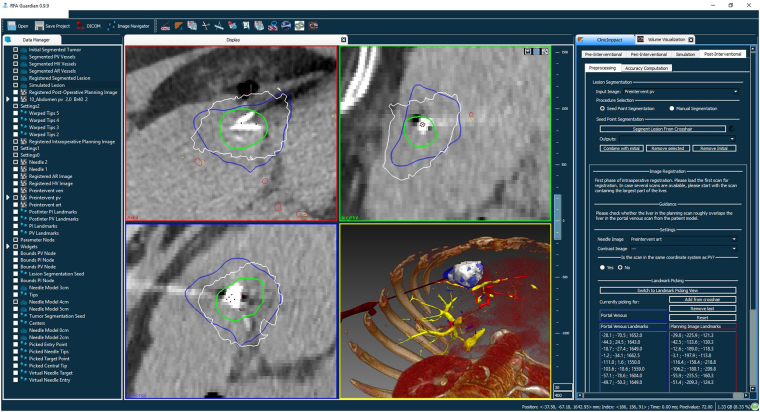
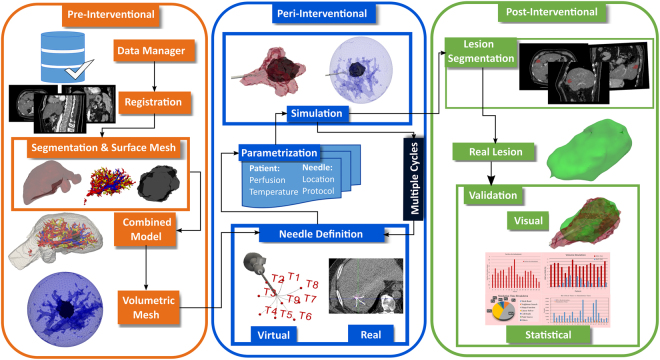
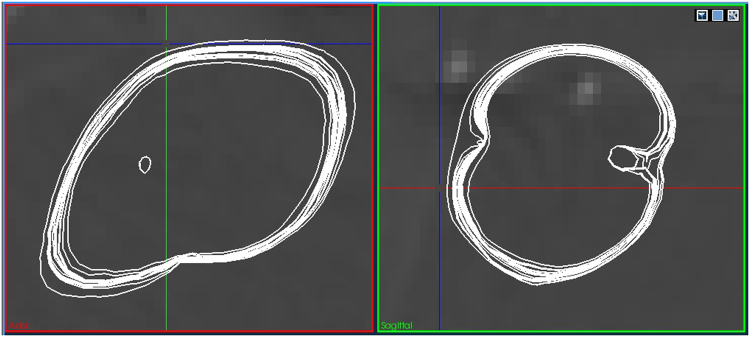
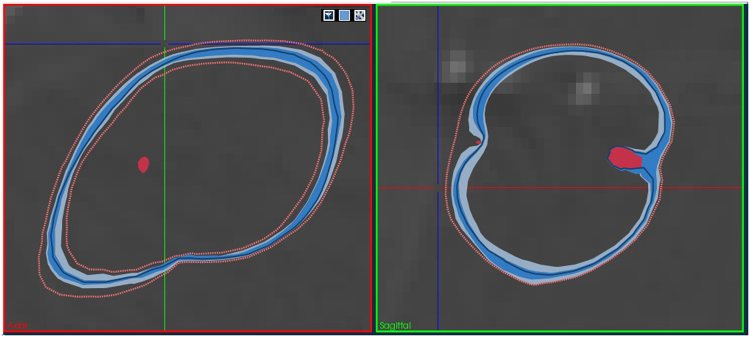
The RFA Guardian is a comprehensive application for high-performance patient-specific simulation of radiofrequency ablation of liver tumors. We address a wide range of usage scenarios. These include pre-interventional planning, sampling of the parameter space for uncertainty estimation, treatment evaluation and, in the worst case, failure analysis. The RFA Guardian is the first of its kind that exhibits sufficient performance for simulating treatment outcomes during the intervention. We achieve this by combining a large number of high-performance image processing, biomechanical simulation and visualization techniques into a generalized technical workflow. Further, we wrap the feature set into a single, integrated application, which exploits all available resources of standard consumer hardware, including massively parallel computing on graphics processing units. This allows us to predict or reproduce treatment outcomes on a single personal computer with high computational performance and high accuracy. The resulting low demand for infrastructure enables easy and cost-efficient integration into the clinical routine. We present a number of evaluation cases from the clinical practice where users performed the whole technical workflow from patient-specific modeling to final validation and highlight the opportunities arising from our fast, accurate prediction techniques.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
