

Anti-inflammatory and antiplatelet effects of non-vitamin K antagonist oral anticoagulants in acute phase of ischemic stroke patients
- PMID: 29335786
- PMCID: PMC5768575
- DOI: 10.1186/s40169-017-0179-9
Anti-inflammatory and antiplatelet effects of non-vitamin K antagonist oral anticoagulants in acute phase of ischemic stroke patients
Abstract
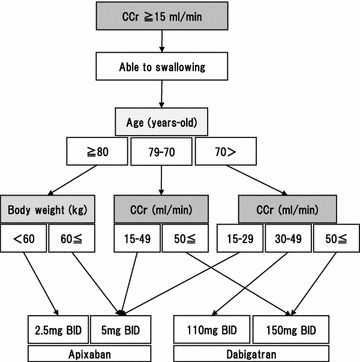
Background: Recently, non-vitamin K antagonist oral anticoagulants such as direct thrombin and direct factor Xa inhibitors have been prescribed for prevention of embolic stroke. While in Japan, argatroban, also a direct thrombin inhibitor, is available for the treatment of atherothrombotic stroke patients. This study aimed to explore whether there is any differences between direct thrombin and direct factor Xa inhibitors regarding the inhibiting effect against thrombogenesis in the clinical setting of acute ischemic stroke.
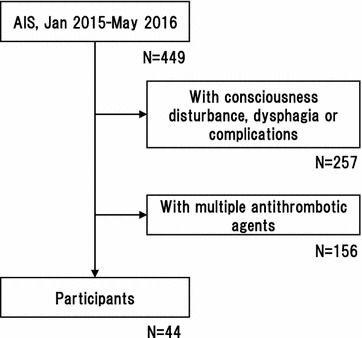
Methods: Acute ischemic stroke patients newly prescribed anti-thrombotic agents were consecutively screened, and 44 patients with single medicine were enrolled (median 72.0 years-old). Blood samples were obtained at 1 and 2 weeks after the medication started. The extent of anticoagulation activity, inflammatory markers and platelet aggregation were assessed. Patients with antiplatelets were used as control.
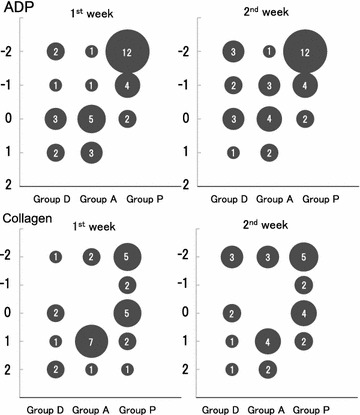
Results: Prescribed antithrombotics were dabigatran (group D: n = 12), apixaban (group A: n = 14) and antiplatelet agents (group P: n = 18). Prevalence of stroke risks and anticoagulation activity were not different between groups D and A. The alteration of inflammatory markers in a week in the group A showed similar trend to those in the group P. The group D presented relatively lower amount of high-sensitive C-reactive protein and higher amount of pentraxin-3 compared with groups A and P. While 88.9% of group P patients showed decreased platelet aggregation activity with adenosine diphosphate, 55.6% of group D and 40.0% of group A presented the inhibition of platelet aggregation activity.
Conclusions: Even in acute ischemic stroke patients, both apixaban and dabigatran equally showed the anticoagulation activity. The reduction of inflammatory response might be prominent in apixaban, whereas the inhibition of platelet aggregation activity might be evident in dabigatran.
Keywords: Blood platelets; Factor Xa; Inflammation; Stroke; Thrombin.
Figures
Similar articles
-
Apixaban, a direct factor Xa inhibitor, inhibits tissue-factor induced human platelet aggregation in vitro: comparison with direct inhibitors of factor VIIa, XIa and thrombin.Thromb Haemost. 2010 Aug;104(2):302-10. doi: 10.1160/TH10-02-0097. Epub 2010 Jun 29. Thromb Haemost. 2010. PMID: 20589316
-
Non-vitamin K antagonist oral anticoagulants in cardiovascular disease management: evidence and unanswered questions.J Clin Pharm Ther. 2014 Apr;39(2):118-35. doi: 10.1111/jcpt.12122. Epub 2014 Jan 3. J Clin Pharm Ther. 2014. PMID: 24383983 Review.
-
Outcome of Secondary Stroke Prevention in Patients Taking Non-Vitamin K Antagonist Oral Anticoagulants.J Stroke Cerebrovasc Dis. 2018 May;27(5):1174-1177. doi: 10.1016/j.jstrokecerebrovasdis.2017.11.032. Epub 2017 Dec 21. J Stroke Cerebrovasc Dis. 2018. PMID: 29276013
-
Point-of-Care Testing of Coagulation in Patients Treated With Non-Vitamin K Antagonist Oral Anticoagulants.Stroke. 2015 Oct;46(10):2741-7. doi: 10.1161/STROKEAHA.115.010148. Epub 2015 Aug 13. Stroke. 2015. PMID: 26272385
-
Novel oral anticoagulants for stroke prevention in atrial fibrillation: focus on apixaban.Adv Ther. 2012 Jun;29(6):491-507. doi: 10.1007/s12325-012-0026-8. Epub 2012 Jun 7. Adv Ther. 2012. PMID: 22684583 Review.
Cited by
-
Comparative Cardioprotective Effectiveness: NOACs vs. Nattokinase-Bridging Basic Research to Clinical Findings.Biomolecules. 2024 Aug 7;14(8):956. doi: 10.3390/biom14080956. Biomolecules. 2024. PMID: 39199344 Free PMC article. Review.
-
Gut microbial dysbiosis, IgA, and Enterococcus in common variable immunodeficiency with immune dysregulation.Microbiome. 2025 Jan 16;13(1):12. doi: 10.1186/s40168-024-01982-y. Microbiome. 2025. PMID: 39819634 Free PMC article.
-
Pathophysiological dynamics in the contact, coagulation, and complement systems during sepsis: Potential targets for nafamostat mesilate.J Intensive Med. 2024 Apr 10;4(4):453-467. doi: 10.1016/j.jointm.2024.02.003. eCollection 2024 Oct. J Intensive Med. 2024. PMID: 39310056 Free PMC article. Review.
-
The Effects of Dabigatran and Rivaroxaban on Markers of Polymorphonuclear Leukocyte Activation.Pharmaceuticals (Basel). 2018 May 14;11(2):46. doi: 10.3390/ph11020046. Pharmaceuticals (Basel). 2018. PMID: 29758017 Free PMC article.
-
Non-Vitamin K Antagonist Oral Anticoagulants Provide Less Adverse Renal Outcomes Than Warfarin In Non-Valvular Atrial Fibrillation: A Systematic Review and MetaAnalysis.J Am Heart Assoc. 2021 Apr 6;10(7):e019609. doi: 10.1161/JAHA.120.019609. Epub 2021 Mar 17. J Am Heart Assoc. 2021. PMID: 33728927 Free PMC article.
References
-
- Okada T, Nakase T, Sasaki M, Ishikawa T. Do the antithrombotic therapy at the time of intracerebral hemorrhage influence clinical outcome? Analysis between the difference of antiplatelet and anticoagulant agents and clinical course. J Stroke Cerebrovasc Dis. 2014;23(7):1781–1788. doi: 10.1016/j.jstrokecerebrovasdis.2014.04.036. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials