

The incidence and significance of periictal apnea in epileptic seizures
- PMID: 29336036
- PMCID: PMC6103445
- DOI: 10.1111/epi.14006
The incidence and significance of periictal apnea in epileptic seizures
Abstract
Objective: The aim of this study was to investigate periictal central apnea as a seizure semiological feature, its localizing value, and possible relationship with sudden unexpected death in epilepsy (SUDEP) pathomechanisms.
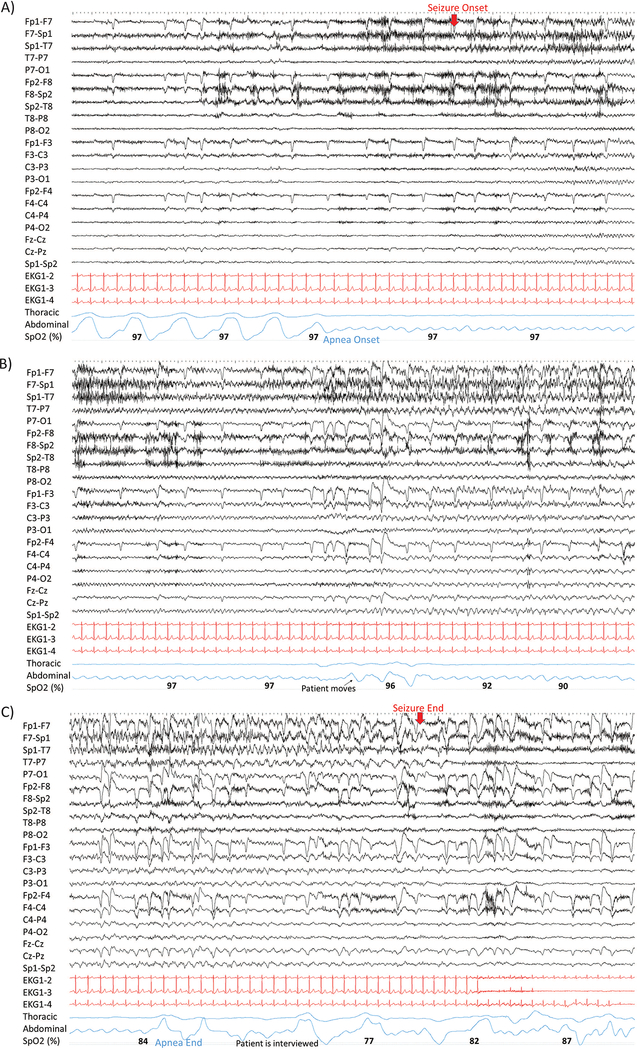
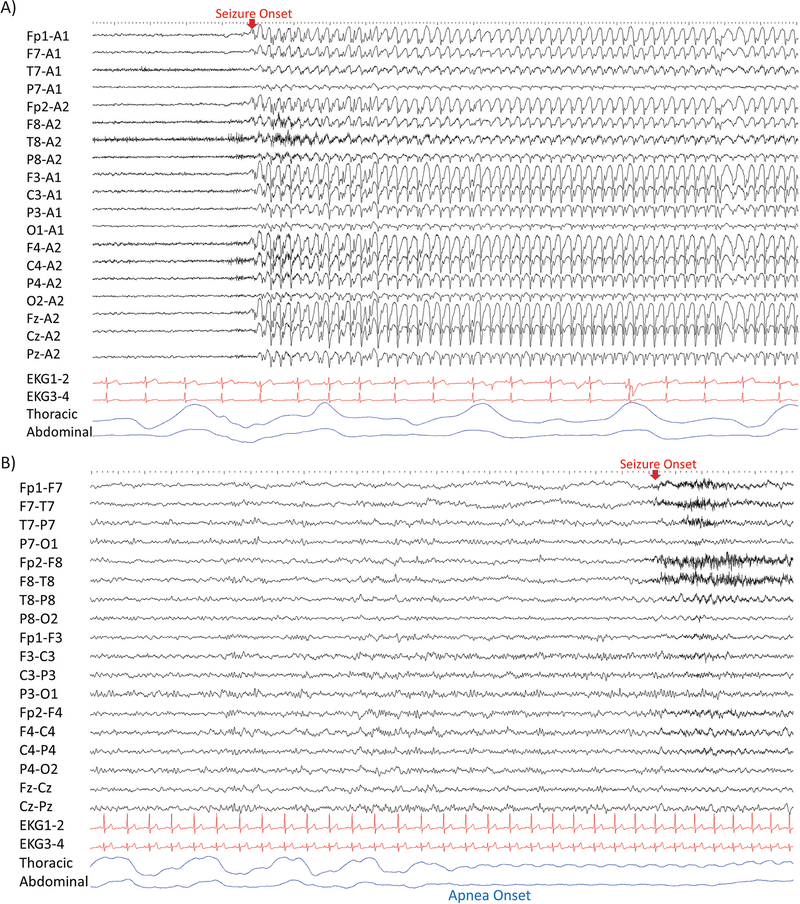
Methods: We prospectively studied polygraphic physiological responses, including inductance plethysmography, peripheral capillary oxygen saturation (SpO2 ), electrocardiography, and video electroencephalography (VEEG) in 473 patients in a multicenter study of SUDEP. Seizures were classified according to the International League Against Epilepsy (ILAE) 2017 seizure classification based on the most prominent clinical signs during VEEG. The putative epileptogenic zone was defined based on clinical history, seizure semiology, neuroimaging, and EEG.
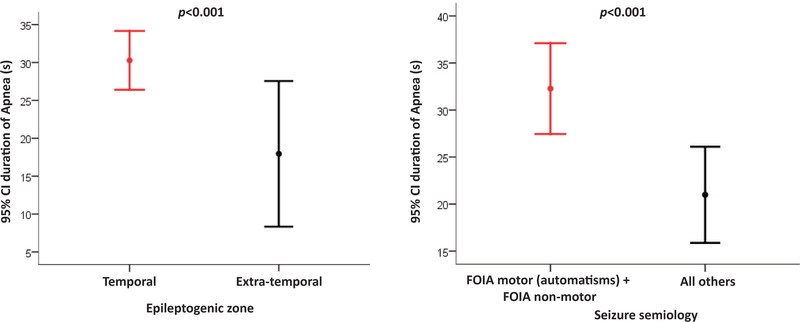
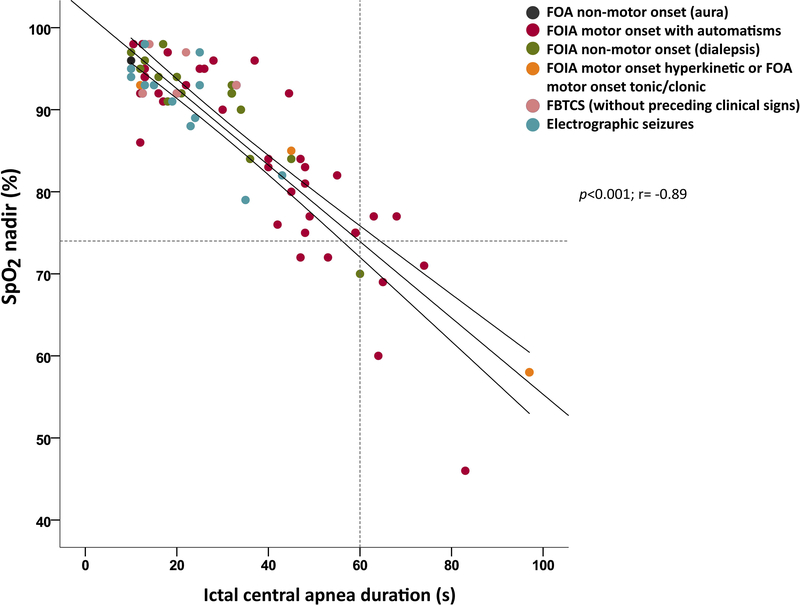
Results: Complete datasets were available in 126 patients in 312 seizures. Ictal central apnea (ICA) occurred exclusively in focal epilepsy (51/109 patients [47%] and 103/312 seizures [36.5%]) (P < .001). ICA was the only clinical manifestation in 16/103 (16.5%) seizures, and preceded EEG seizure onset by 8 ± 4.9 s, in 56/103 (54.3%) seizures. ICA ≥60 s was associated with severe hypoxemia (SpO2 <75%). Focal onset impaired awareness (FOIA) motor onset with automatisms and FOA nonmotor onset semiologies were associated with ICA presence (P < .001), ICA duration (P = .002), and moderate/severe hypoxemia (P = .04). Temporal lobe epilepsy was highly associated with ICA in comparison to extratemporal epilepsy (P = .001) and frontal lobe epilepsy (P = .001). Isolated postictal central apnea was not seen; in 3/103 seizures (3%), ICA persisted into the postictal period.
Significance: ICA is a frequent, self-limiting semiological feature of focal epilepsy, often starting before surface EEG onset, and may be the only clinical manifestation of focal seizures. However, prolonged ICA (≥60 s) is associated with severe hypoxemia and may be a potential SUDEP biomarker. ICA is more frequently seen in temporal than extratemporal seizures, and in typical temporal seizure semiologies. ICA rarely persists after seizure end. ICA agnosia is typical, and thus it may remain unrecognized without polygraphic measurements that include breathing parameters.
Keywords: apnea; breathing; seizures; sudden unexpected death in epilepsy; temporal epilepsy.
Wiley Periodicals, Inc. © 2018 International League Against Epilepsy.
Figures
Comment in
-
SUDEP: When the Nightmare Becomes the Reality.Epilepsy Curr. 2018 Jul-Aug;18(4):227-230. doi: 10.5698/1535-7597.18.4.227. Epilepsy Curr. 2018. PMID: 30254515 Free PMC article. No abstract available.
References
-
- Ryvlin P, Nashef L, Lhatoo SD, et al. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol 2013;12:966–977. - PubMed
-
- James MR, Marshall H, Carew-McColl M. Pulse oximetry during apparent tonic-clonic seizures. Lancet 1991;337:394–395. - PubMed
-
- Blum AS, Ives JR, Goldberger AL, et al. Oxygen desaturations triggered by partial seizures: implications for cardiopulmonary instability in epilepsy. Epilepsia 2000;41:536–541. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
