

Neurosensory Deficits Vary as a Function of Point of Care in Pediatric Mild Traumatic Brain Injury
- PMID: 29336197
- PMCID: PMC5953216
- DOI: 10.1089/neu.2017.5340
Neurosensory Deficits Vary as a Function of Point of Care in Pediatric Mild Traumatic Brain Injury
Abstract
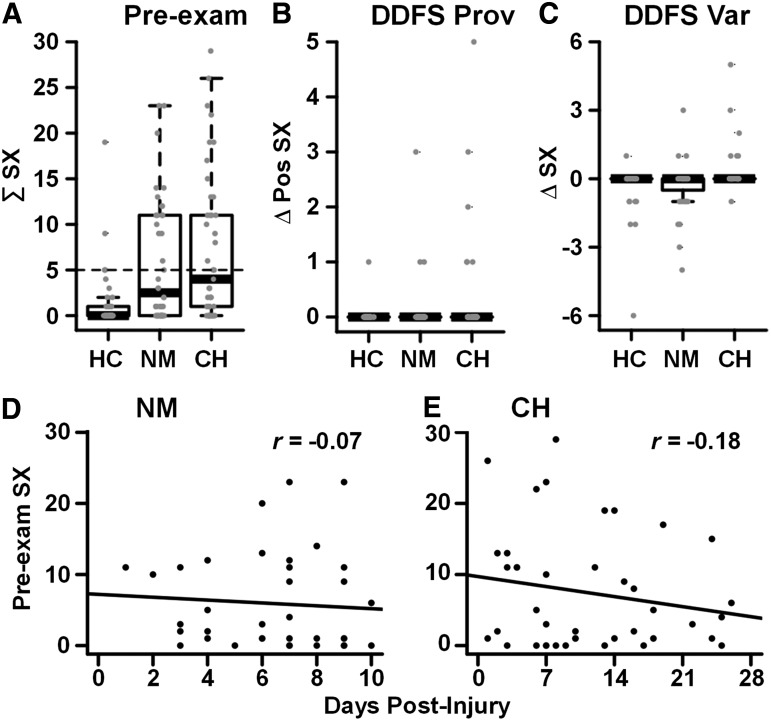
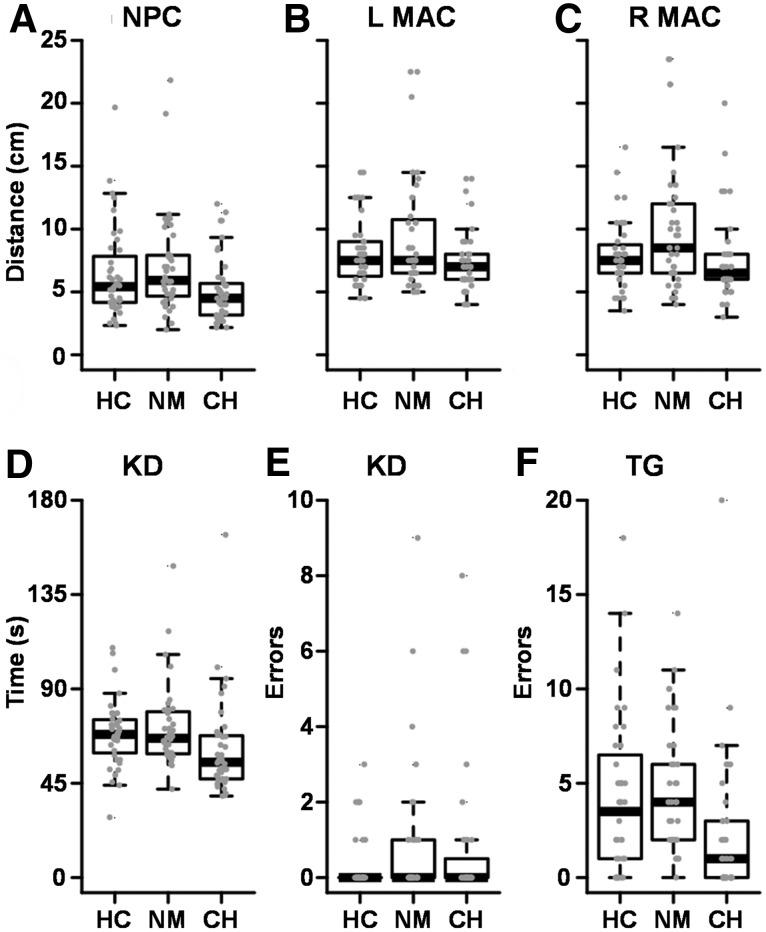
Neurosensory abnormalities are frequently observed following pediatric mild traumatic brain injury (pmTBI) and may underlie the expression of several common concussion symptoms and delay recovery. Importantly, active evaluation of neurosensory functioning more closely approximates real-world (e.g., physical and academic) environments that provoke symptom worsening. The current study determined whether symptom provocation (i.e., during neurosensory examination) improved classification accuracy relative to pre-examination symptom levels and whether symptoms varied as a function of point of care. Eighty-one pmTBI were recruited from the pediatric emergency department (PED; n = 40) or outpatient concussion clinic (n = 41), along with matched (age, sex, and education) healthy controls (HC; n = 40). All participants completed a brief (∼ 12 min) standardized neurosensory examination and clinical questionnaires. The magnitude of symptom provocation upon neurosensory examination was significantly higher for concussion clinic than for PED patients. Symptom provocation significantly improved diagnostic classification accuracy relative to pre-examination symptom levels, although the magnitude of improvement was modest, and was greater in the concussion clinic. In contrast, PED patients exhibited worse performance on measures of balance, vision, and oculomotor functioning than the concussion clinic patients, with no differences observed between both samples and HC. Despite modest sample sizes, current findings suggest that point of care represents a critical but highly under-studied variable that may influence outcomes following pmTBI. Studies that rely on recruitment from a single point of care may not generalize to the entire pmTBI population in terms of how neurosensory deficits affect recovery.
Keywords: neurosensory; ocular motor; pmTBI; recovery; vestibular; vision.
Conflict of interest statement
No competing financial interests exist.
Figures

References
-
- Marin J.R., Weaver M.D., Yealy D.M., and Mannix R.C. (2014). Trends in visits for traumatic brain injury to emergency departments in the United States. JAMA 311, 1917–1919 - PubMed
-
- Zemek R.L., Grool A.M., Duque D.R., DeMatteo C., Rothman L., Benchimol E.I., Guttmann A., and Macpherson A.K. (2016). Annual and seasonal trends in ambulatory visits for pediatric concussion in Ontario between 2003 and 2013. J. Pediatr. 181, 222–228 - PubMed
-
- Zemek R., Barrowman N., Freedman S.B., Gravel J., Gagnon I., McGahern C., Aglipay M., Sangha G., Boutis K., Beer D., Craig W., Burns E., Farion K.J., Mikrogianakis A., Barlow K., Dubrovsky A.S., Meeuwisse W., Gioia G., Meehan W.P., III, Beauchamp M.H., Kamil Y., Grool A.M., Hoshizaki B., Anderson P., Brooks B.L., Yeates K.O., Vassilyadi M., Klassen T., Keightley M., Richer L., DeMatteo C., and Osmond M.H. (2016). Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA 315, 1014–1025 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
