

Transurethral resection of the prostate provides more favorable clinical outcomes compared with conservative medical treatment in patients with urinary retention caused by benign prostatic obstruction
- PMID: 29338688
- PMCID: PMC5771192
- DOI: 10.1186/s12877-018-0709-3
Transurethral resection of the prostate provides more favorable clinical outcomes compared with conservative medical treatment in patients with urinary retention caused by benign prostatic obstruction
Abstract
Background: To evaluate the long-term surgical outcomes of patients with urinary retention (UR) caused by a benign prostatic obstruction (BPO) who underwent transurethral resection of the prostate (TURP), and compare their outcomes with those of patients who received medication without surgical intervention.
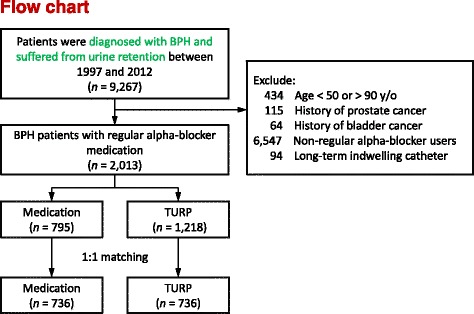
Methods: This retrospective cohort study analyzed claims data collected during the period of 1997-2012 from Taiwan's National Health Insurance Research Database. We examined geriatric adverse events among patients who had received a diagnosis of symptomatic benign prostatic hyperplasia and whom experienced UR, and compared those who received TURP and medication only. Primary outcomes included urinary tract infection (UTI), UR, inguinal hernia, hemorrhoids, stroke, acute myocardial infarction, and bony fracture. We excluded patients who had concomitant prostate cancer, bladder cancer, or a long-term urinary catheter indwelling, as well as those who did not receive α-blocker medication regularly. Those aged <50 or >90 years were also excluded. The enrolled patients were categorized into TURP (n = 1218) and medication only (n = 795) groups. After 1:1 propensity score matching, we recorded and compared patients' characteristics, postoperative clinical outcomes, and geriatric adverse events.
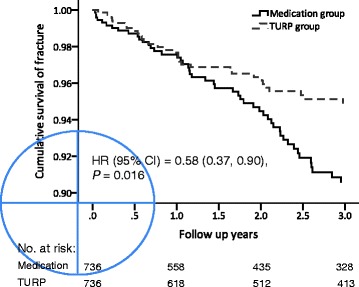
Results: The TURP cohort had a lower incidence of UTI and UR during the postoperative follow-up period from 2 months to 3 years than did the medication only group (20.7% vs. 28.9% and 12.5% vs. 27.6%, respectively, p < 0.001). The life-long bone fracture incidence was also lower in the TURP cohort (7.9% vs. 9.2%, p = 0.048). The incidence of other outcomes during the postoperative follow-up period did not differ between the two groups.
Conclusions: Compared with conservative treatment, TURP provides more favorable clinical outcomes in patients with UR caused by BPO. Patients who underwent TURP had a lower risk of UTI, repeat UR episodes, and emergent bony fracture. Thus, early surgical intervention should be considered for such patients.
Keywords: Alfa-blocker; Benign prostate hyperplasia; Outcome; Prostatectomy; Urine retention.
Conflict of interest statement
Ethics approval and consent to participate
We obtained written consent from the participants. The protocol of this project was approved by the Ethics Committee on Chang Gung Memorial Hospital Ethics Board at the CGMH, Taiwan, 104-7627B.
Competing interests
The authors declare that they have no competing interests.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Selius BA, Subedi R. Urinary retention in adults: diagnosis and initial management. Am Fam Physician. 2008;77(5):643–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
