

Evolution of Intravitreal Therapy for Retinal Diseases-From CMV to CNV: The LXXIV Edward Jackson Memorial Lecture
- PMID: 29339063
- PMCID: PMC6014888
- DOI: 10.1016/j.ajo.2017.12.019
Evolution of Intravitreal Therapy for Retinal Diseases-From CMV to CNV: The LXXIV Edward Jackson Memorial Lecture
Abstract
Purpose: To present the evolution of intravitreal therapy for retinal diseases and its impact on clinical practice.
Design: Retrospective literature review and personal perspective.
Methods: Retrospective literature review and personal perspective.
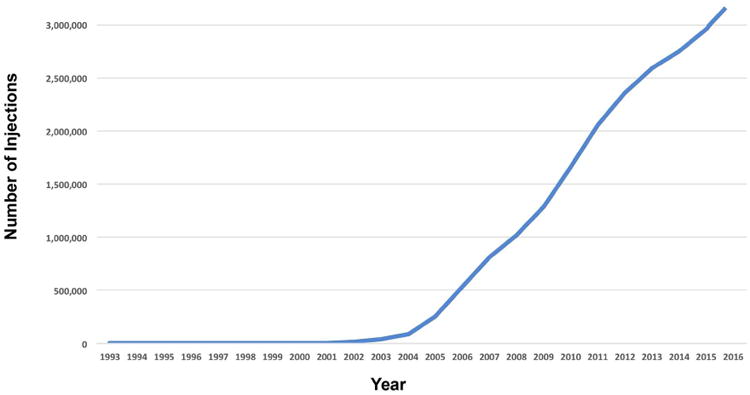
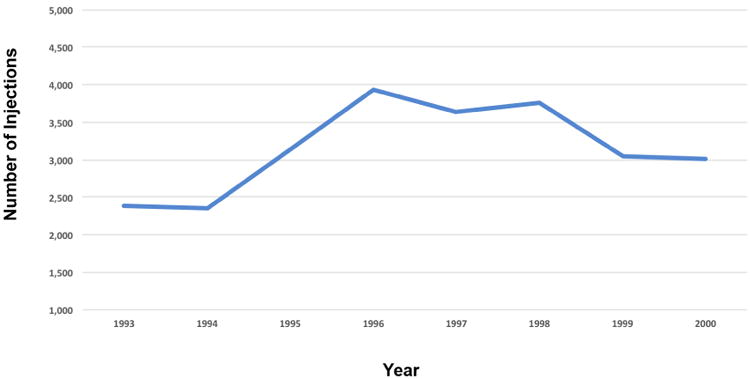
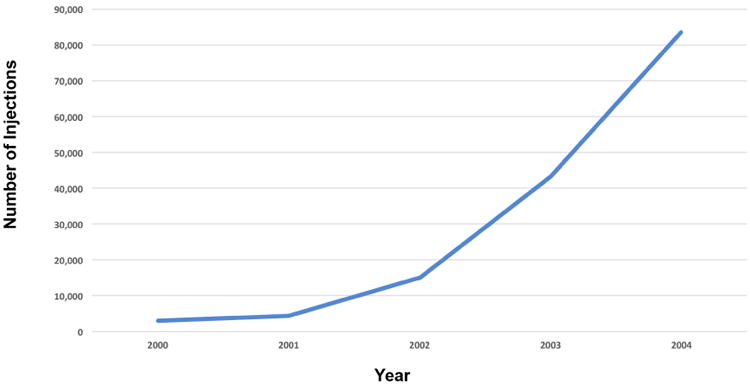
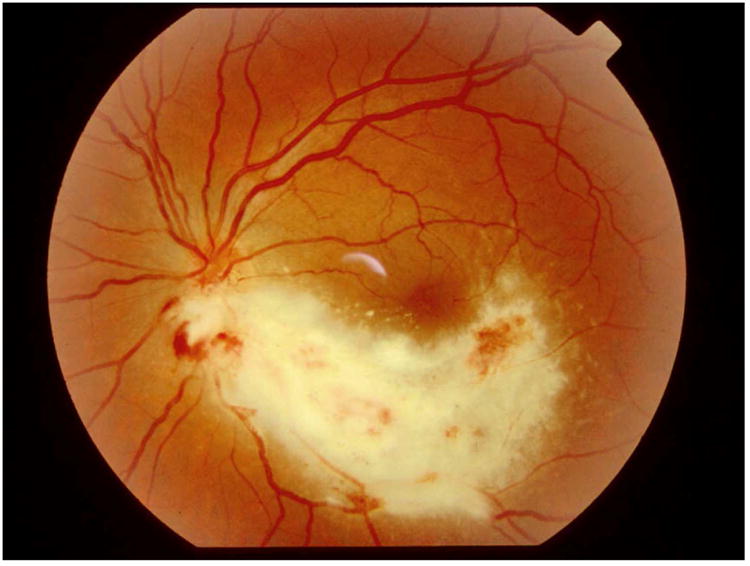
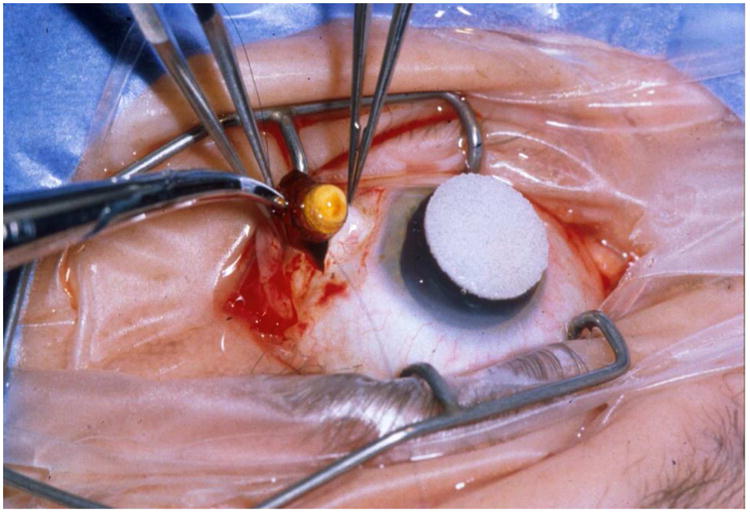
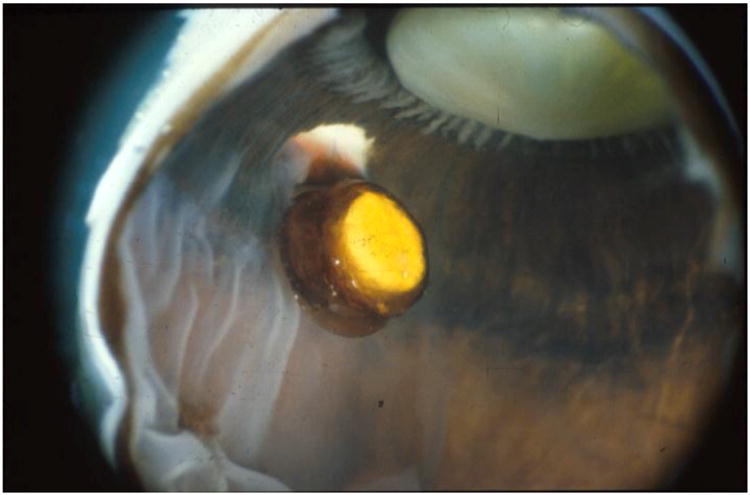
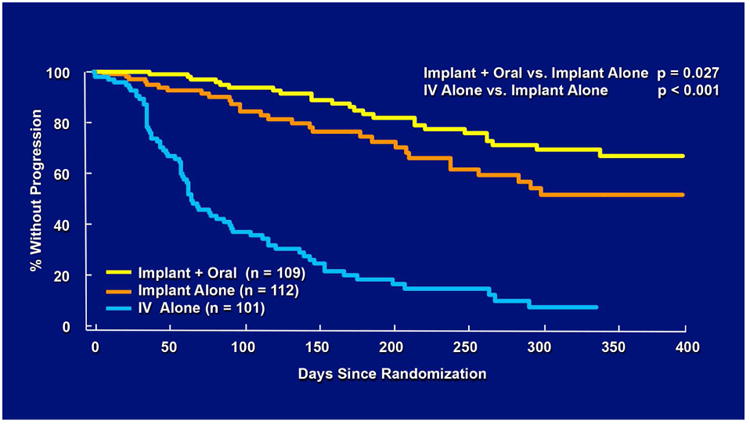
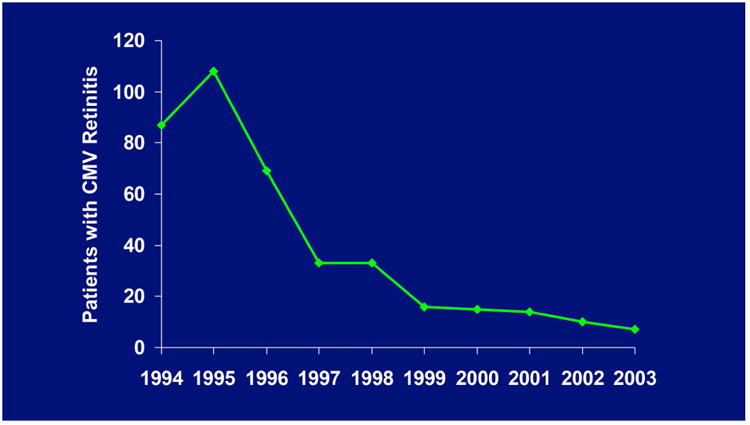
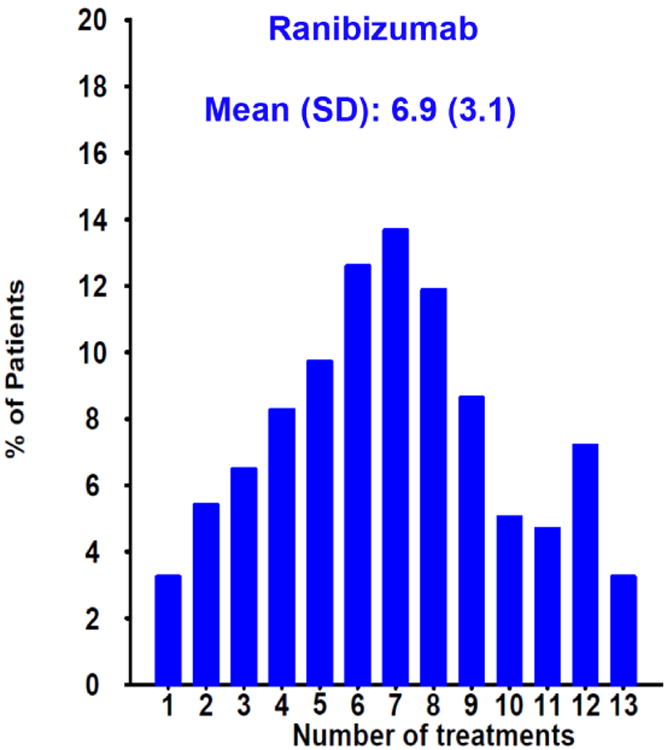
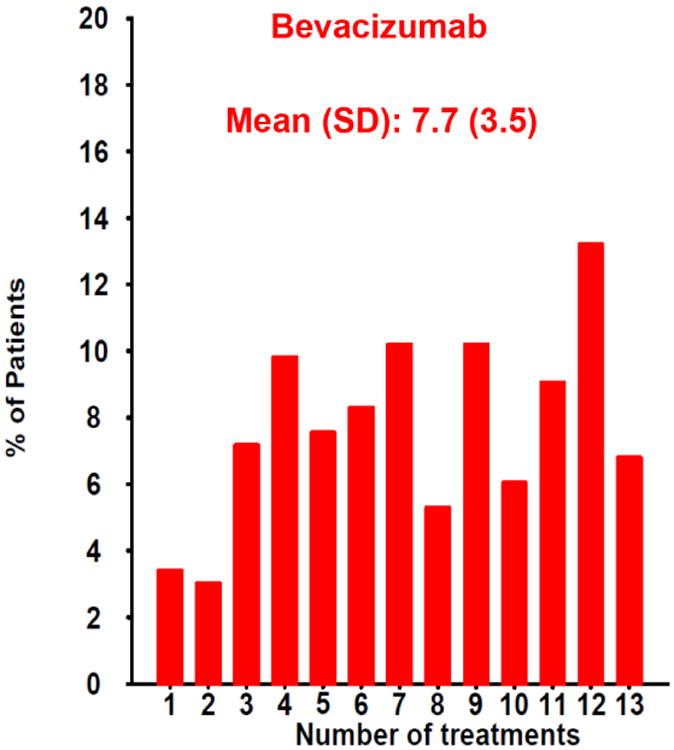
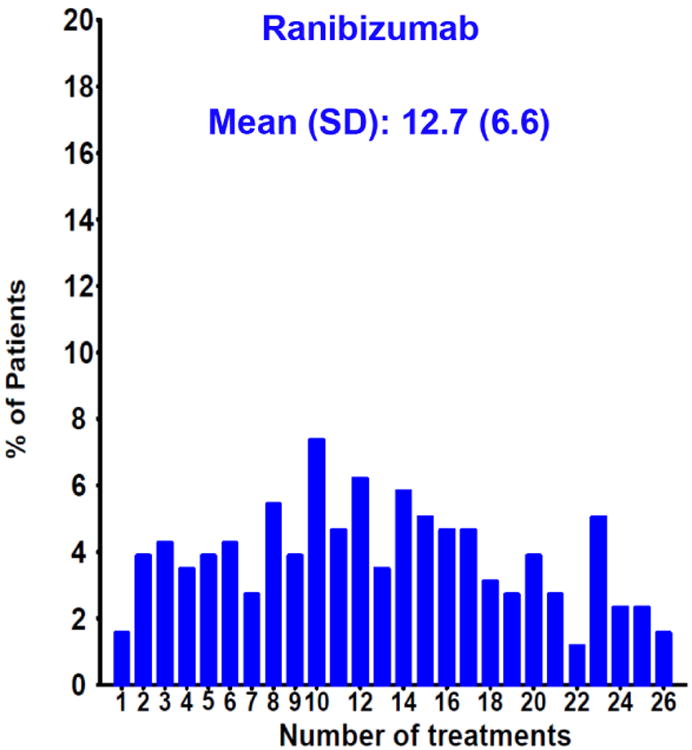
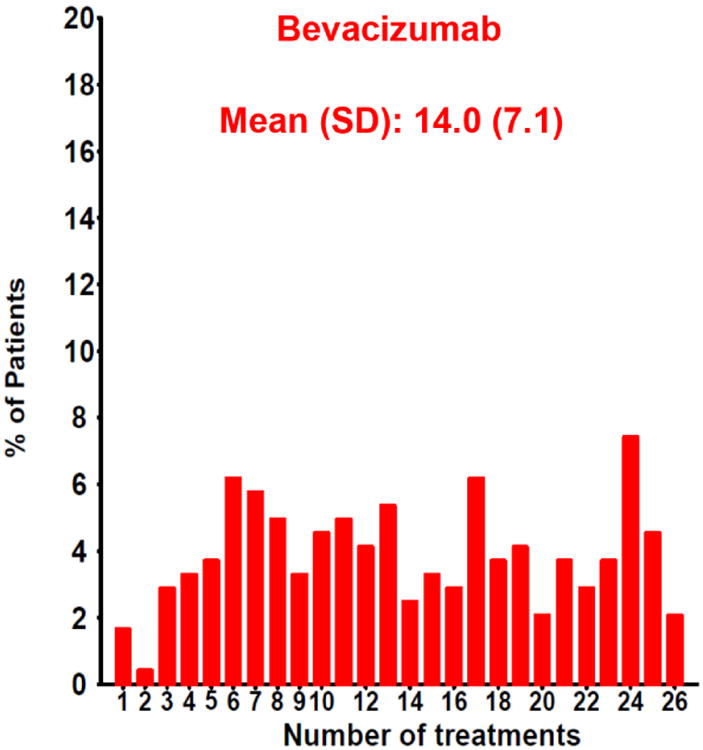
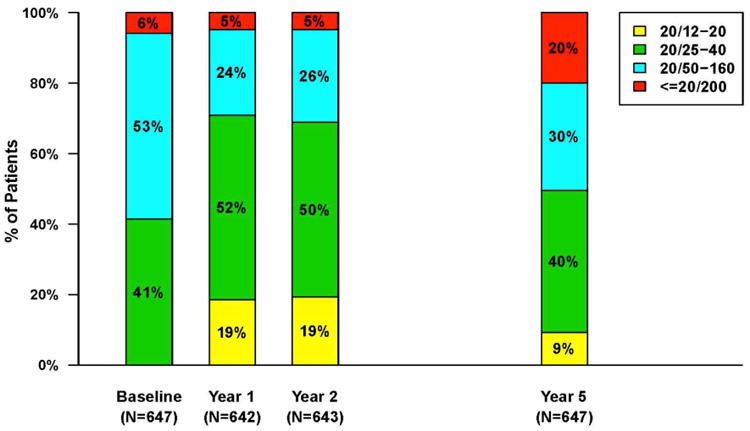
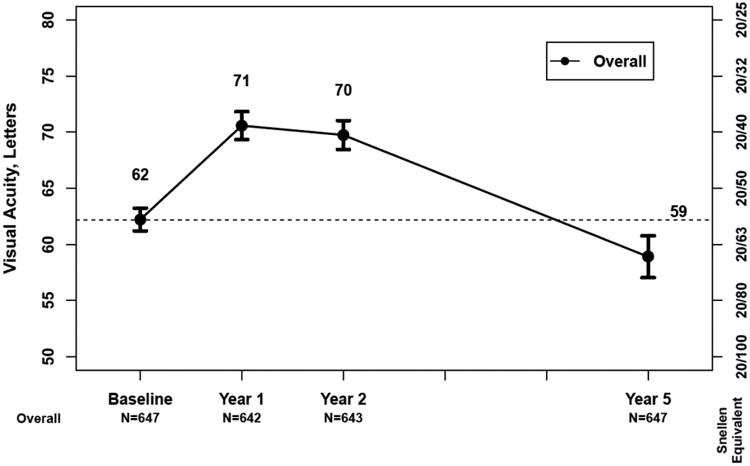
Results: Pharmacotherapeutic advances in retinal disease have been remarkable over the last 25 years. Almost all of the new drugs developed have required intravitreal administration to be highly effective, leading to an exponential increase in the annual number of intravitreal injections given. The use of intravitreal antibiotic injections to treat endophthalmitis, usually on a one-time basis, first familiarized ophthalmologists with this method of drug delivery. Ganciclovir was the first widely available, relatively inexpensive compounded drug that was used for repeat intravitreal injection to treat a chronic retinal disease, followed by triamcinolone for diabetic macular edema and bevacizumab for neovascular age-related macular degeneration. Ganciclovir was formulated for sustained-release drug delivery to avoid frequent intravitreal injections, a goal that has been more elusive for anti-VEGF drugs. Political obstacles encountered while conducting some of the trials to evaluate these treatments were substantial. Addressing the issues they raised led to important national policy changes that will impact the conduct of future clinical trials. The first comparative efficacy trial of intravitreal therapies was the Comparison of AMD Treatments Trials (CATT). The primary results from CATT and the many publications that followed continue to shape the use of intravitreal therapy today.
Conclusion: Intravitreal therapy has proven highly effective for the treatment of many retinal diseases. The treatment burden for patients from numerous injections, the cost to health care systems, and the impact on workflows in clinical practice have been substantial. Efforts to develop effective intravitreal therapies with reduced treatment burden and cost are ongoing.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interests: None
Figures
References
-
- Williams G. Intravitreal injections: health policy implications. Review of Ophthalmology. 2014;(June) https://www.reviewofophthalmology.com/article/ivt-injections-health-poli....
-
- RBRVS DataManager Online. Copyright American Medical Association
-
- Machemer R, Aaberg TM. Vitrectomy. New York: Grune & Stratton; 1979.
-
- Peyman GA, Herbst R. Bacterial endophthalmitis Treatment with intraocular injection of gentamicin and dexamethasone. Arch Ophthalmol. 1974;91:416–418. - PubMed
-
- May DR, Ericson ES, Peyman GA, Axelrod AJ. Intraocular injection of gentamicin. Single injection therapy of experimental bacterial endophthalmitis. Arch Ophthalmol. 1974;91:487–489. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
