

Human airway branch variation and chronic obstructive pulmonary disease
- PMID: 29339516
- PMCID: PMC5798356
- DOI: 10.1073/pnas.1715564115
Human airway branch variation and chronic obstructive pulmonary disease
Abstract
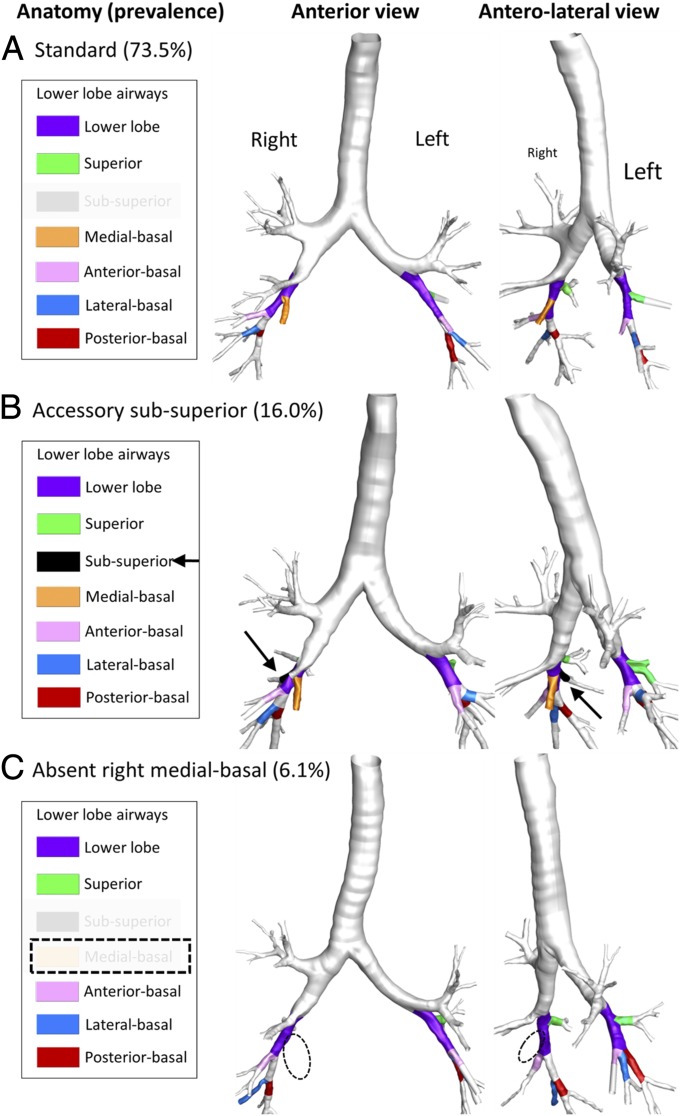
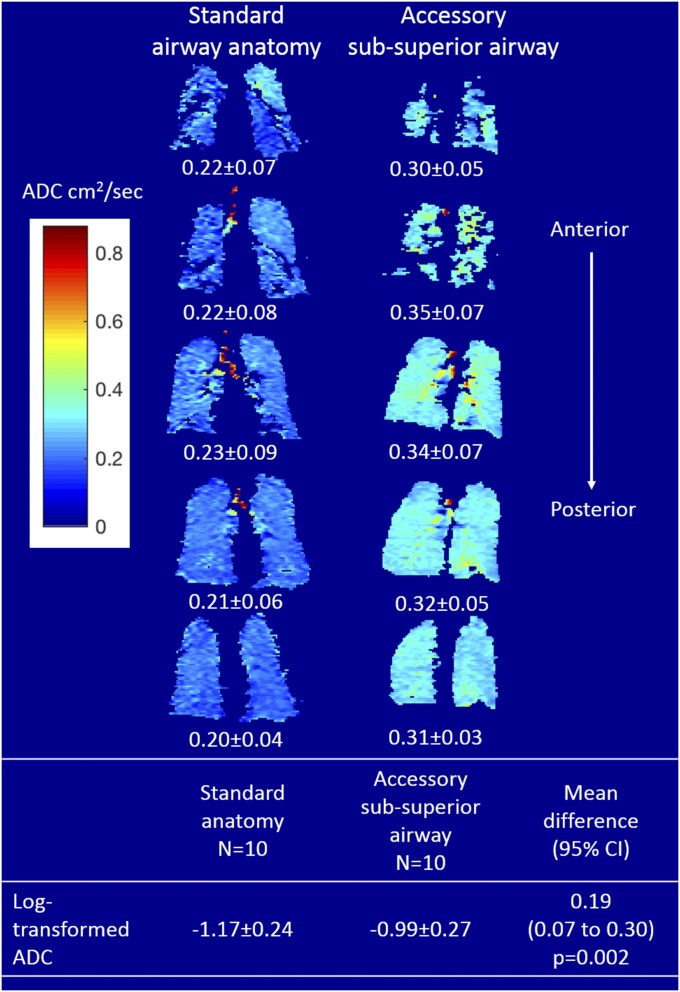
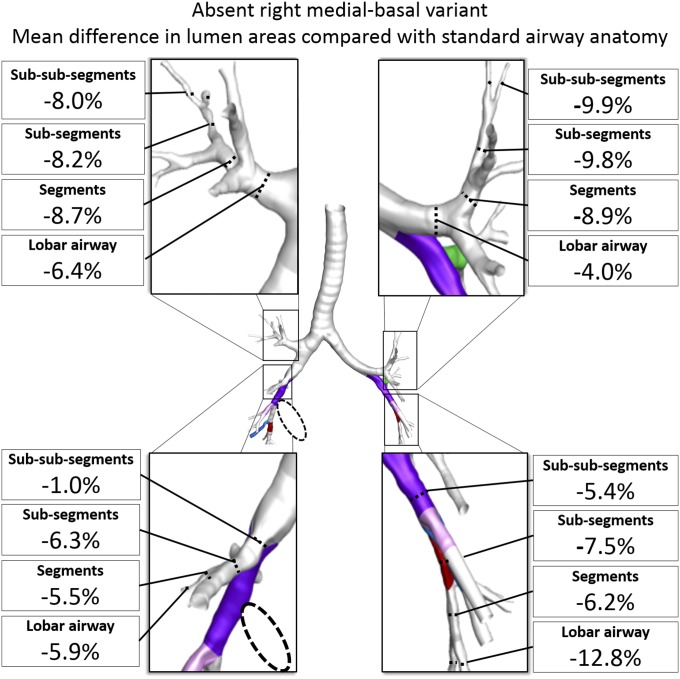
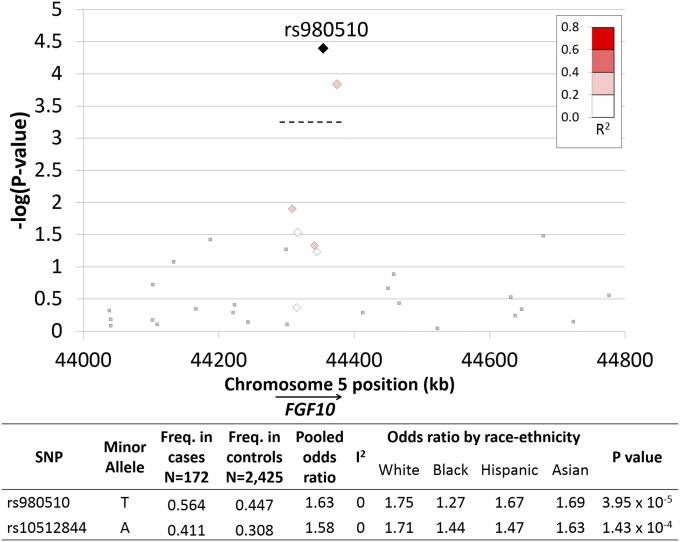
Susceptibility to chronic obstructive pulmonary disease (COPD) beyond cigarette smoking is incompletely understood, although several genetic variants associated with COPD are known to regulate airway branch development. We demonstrate that in vivo central airway branch variants are present in 26.5% of the general population, are unchanged over 10 y, and exhibit strong familial aggregation. The most common airway branch variant is associated with COPD in two cohorts (n = 5,054), with greater central airway bifurcation density, and with emphysema throughout the lung. The second most common airway branch variant is associated with COPD among smokers, with narrower airway lumens in all lobes, and with genetic polymorphisms within the FGF10 gene. We conclude that central airway branch variation, readily detected by computed tomography, is a biomarker of widely altered lung structure with a genetic basis and represents a COPD susceptibility factor.
Keywords: airway branching; chronic obstructive pulmonary disease; computed tomography; fibroblast growth factor.
Conflict of interest statement
Conflict of interest statement: E.A.H. is co-founder and share-holder in VIDA Diagnostics, which commercialized the software used to assess lung volumes and percent emphysema (but not airway anatomy) in this study.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- N01HC95161/HL/NHLBI NIH HHS/United States
- N01HC95168/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- K24 HL137013/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01HC95163/HL/NHLBI NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- R35 HL135834/HL/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- N01HC95165/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- U01 HL114494/HL/NHLBI NIH HHS/United States
- N01HC95167/HL/NHLBI NIH HHS/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- R01 HL121270/HL/NHLBI NIH HHS/United States
- R01 HL130506/HL/NHLBI NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- HHSN268200900020C/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- N01HC95166/HL/NHLBI NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
