

APOL1 Genotype and Renal Function of Black Living Donors
- PMID: 29339549
- PMCID: PMC5875947
- DOI: 10.1681/ASN.2017060658
APOL1 Genotype and Renal Function of Black Living Donors
Abstract
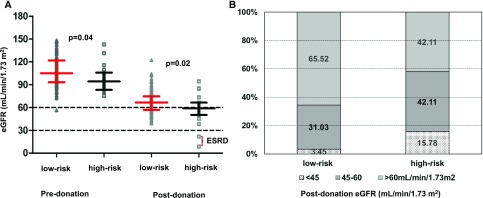
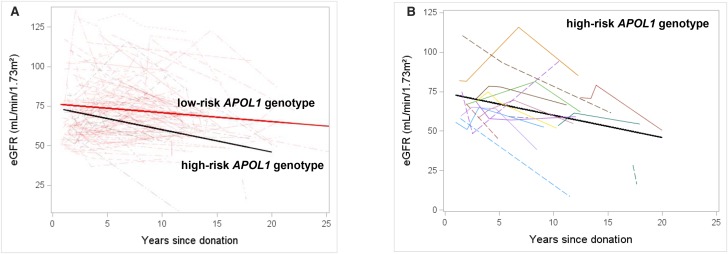
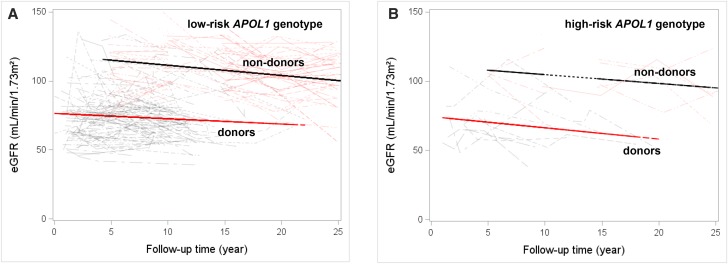
Black living kidney donors are at higher risk of developing kidney disease than white donors. We examined the effect of the APOL1 high-risk genotype on postdonation renal function in black living kidney donors and evaluated whether this genotype alters the association between donation and donor outcome. We grouped 136 black living kidney donors as APOL1 high-risk (two risk alleles; n=19; 14%) or low-risk (one or zero risk alleles; n=117; 86%) genotype. Predonation characteristics were similar between groups, except for lower mean±SD baseline eGFR (CKD-EPI equation) in donors with the APOL1 high-risk genotype (98±17 versus 108±20 ml/min per 1.73 m2; P=0.04). At a median of 12 years after donation, donors with the APOL1 high-risk genotype had lower eGFR (57±18 versus 67±15 ml/min per 1.73 m2; P=0.02) and faster decline in eGFR after adjusting for predonation eGFR (1.19; 95% confidence interval, 0 to 2.3 versus 0.4; 95% confidence interval, 0.1 to 0.7 ml/min per 1.73 m2 per year, P=0.02). Two donors developed ESRD; both carried the APOL1 high-risk genotype. In a subgroup of 115 donors matched to 115 nondonors by APOL1 genotype, we did not find a difference between groups in the rate of eGFR decline (P=0.39) or any statistical interaction by APOL1 status (P=0.92). In conclusion, APOL1 high-risk genotype in black living kidney donors associated with greater decline in postdonation kidney function. Trajectory of renal function was similar between donors and nondonors. The association between APOL1 high-risk genotype and poor renal outcomes in kidney donors requires validation in a larger study.
Keywords: human genetics; kidney donation; renal function.
Copyright © 2018 by the American Society of Nephrology.
Figures

Comment in
-
Evaluation of Potential Living Kidney Donors in the APOL1 Era.J Am Soc Nephrol. 2018 Apr;29(4):1079-1081. doi: 10.1681/ASN.2018020137. Epub 2018 Mar 9. J Am Soc Nephrol. 2018. PMID: 29523593 Free PMC article. No abstract available.
References
-
- Terasaki PI, Cecka JM, Gjertson DW, Takemoto S: High survival rates of kidney transplants from spousal and living unrelated donors. N Engl J Med 333: 333–336, 1995 - PubMed
-
- Doshi MD, Goggins MO, Li L, Garg AX: Medical outcomes in African American live kidney donors: A matched cohort study. Am J Transplant 13: 111–118, 2013 - PubMed
-
- Mjøen G, Hallan S, Hartmann A, Foss A, Midtvedt K, Øyen O, et al. : Long-term risks for kidney donors. Kidney Int 86: 162–167, 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
