

Complex Reconstruction with Flaps After Abdominoperineal Resection and Groin Dissection for Anal Squamous Cell Carcinoma: A Difficult Case Involving Many Specialities
- PMID: 29339717
- PMCID: PMC5782837
- DOI: 10.12659/ajcr.906818
Complex Reconstruction with Flaps After Abdominoperineal Resection and Groin Dissection for Anal Squamous Cell Carcinoma: A Difficult Case Involving Many Specialities
Abstract
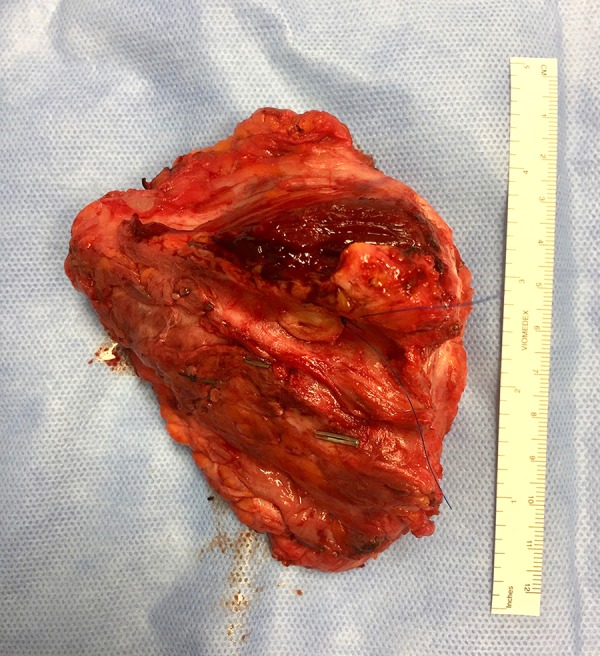
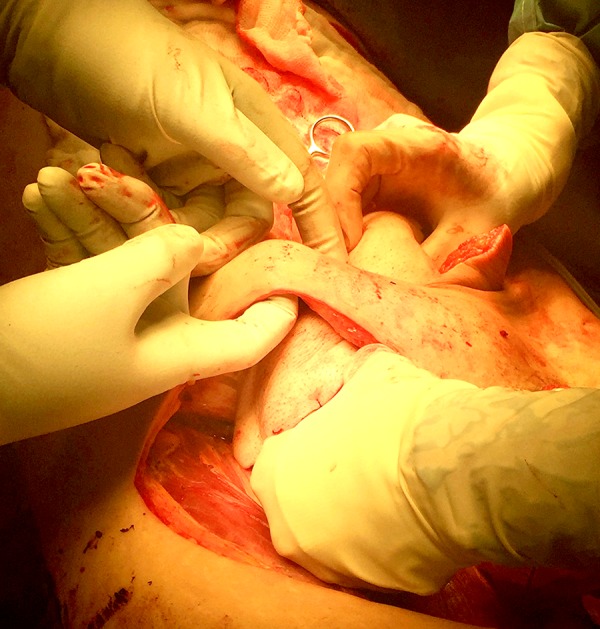
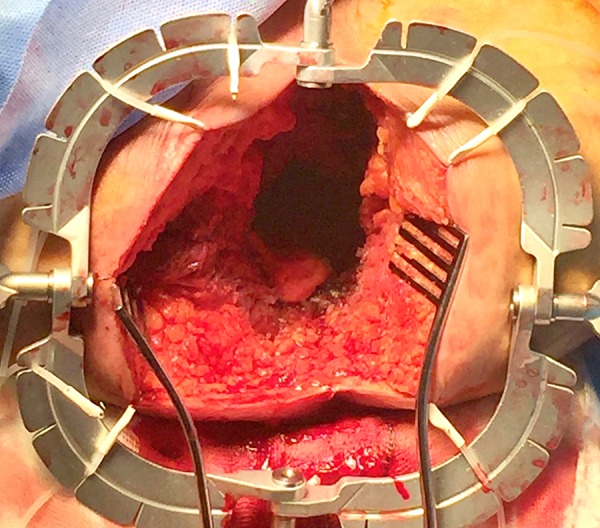
BACKGROUND Anal squamous cell carcinoma accounts for about 2-4% of all lower gastrointestinal malignancies, with a distant disease reported in less than 5%. Although surgical treatment is rarely necessary, this often involve large dissections and difficult reconstructive procedures. CASE REPORT We present a complex but successful case of double-flap reconstruction after abdominoperineal resection and groin dissection for anal squamous cell carcinoma (cT3N3M0) with metastatic right inguinal lymph nodes and ipsilateral threatening of femoral vessels. A multi-specialty team was involved in the operation. A vascular and plastic surgeon performed the inguinal dissection with en bloc excision of the saphenous magna and a cuff of the femoral vein, while colorectal surgeons carried out the abdominoperineal excision. The 2 large tissue gaps at the groin and perineum were covered with an oblique rectus abdominis myocutaneous flap and a gluteal lotus flap, respectively. A partially absorbable mesh was placed at the level of the anterior sheath in order to reinforce the abdominal wall, whereas an absorbable mesh was used as a bridge for the dissected pelvic floor muscles. The post-operative period was uneventful and the follow-up at 5 months showed good results. CONCLUSIONS An early diagnosis along with new techniques of radiochemotherapy allow patients to preserve their sphincter function. However, a persistent or recurrent disease needs major operations, which often involve a complex reconstruction. Good team-work and experience in specialized fields give the opportunity to make the best choices to perform critical steps during the management of complex cases.
Conflict of interest statement
Figures







References
-
- Johnson LG, Madeleine MM, Newcomer LM, et al. Anal cancer incidence and survival: The surveillance, epidemiology and end results experience, 1973– 2000. Cancer. 2004;101:281288. - PubMed
-
- Wilkinson JR, Morris EJ, Downing A, et al. The rising incidence of anal cancer in England 1990–2010: A population-based study. Colorectal Dis. 2014;16(7):O234–39. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
