

Economic Consequences of an Implanted Neuroprosthesis in Subjects with Spinal Cord Injury for Restoration of an Effective Cough
- PMID: 29339903
- PMCID: PMC5562035
- DOI: 10.1310/sci2303-271
Economic Consequences of an Implanted Neuroprosthesis in Subjects with Spinal Cord Injury for Restoration of an Effective Cough
Abstract
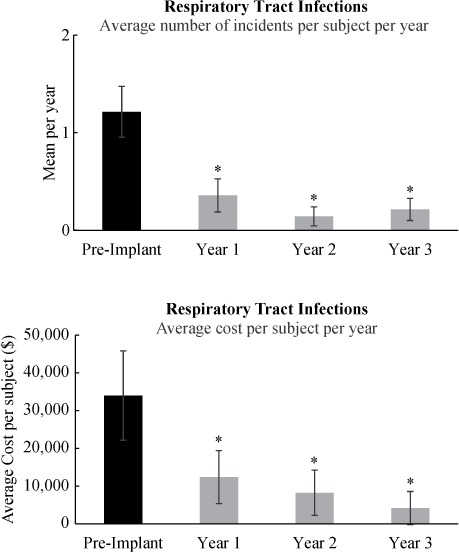
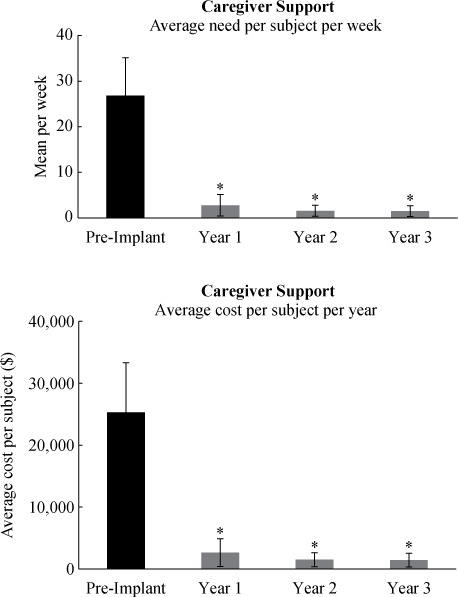
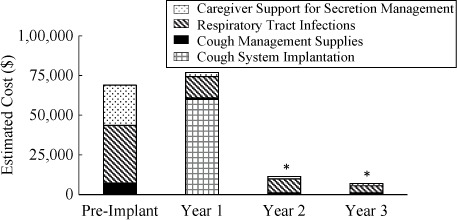
Objective: To determine if an implanted neuroprosthesis for restoration of an effective cough is less costly than conventional methods of respiratory management. Methods: Nonrandomized clinical trial of participants (N = 14) with spinal cord injury (SCI) using the Cough Stimulator device in the inpatient hospital setting for Cough Stimulator implantation and outpatient hospital or residence for follow-up. A neuroprosthesis was implanted for restoration of an effective cough. The annual costs associated with respiratory management, without (pre implantation) and with (post implantation) the neuroprosthesis, were examined over a 4-year period. Results: The total cost related to implantation of the Cough Stimulator was $59,891, with no maintenance costs over subsequent years. The incidence of respiratory tract infections and the need for caregiver support fell significantly following implantation. The costs associated with respiratory tract infections fell significantly from a mean of $36,406 ± 11,855/year to $13,284 ± 7,035/year (p < .05) pre and post implantation, respectively. Costs fell further to $8,817 ± 5,990 and $4,467 ± 4,404 following the 2nd and 3rd years post implantation (p < .05), respectively. The costs associated with caregiver support fell significantly from $25,312 ± 8,019/year to $2,630 ± 2,233/year (p < .05) pre and post implantation, respectively, and remained low in subsequent years (p < .05). Other costs related to secretion management fell significantly and remained low in subsequent years (p < .05). Break-even analysis demonstrated that this point was reached in the first year. Conclusion: The results of this investigation demonstrate that implantation and use of the Cough Stimulator resulted in significant reductions in the overall costs of respiratory management in this patient population.
Keywords: cough; economics; expiratory muscles; rehabilitation; spinal cord stimulation.
Figures
Similar articles
-
Lower thoracic spinal cord stimulation to restore cough in patients with spinal cord injury: results of a National Institutes of Health-Sponsored clinical trial. Part II: clinical outcomes.Arch Phys Med Rehabil. 2009 May;90(5):726-32. doi: 10.1016/j.apmr.2008.11.014. Arch Phys Med Rehabil. 2009. PMID: 19406290 Free PMC article. Clinical Trial.
-
Economic consequences of an implanted neuroprosthesis for bladder and bowel management.Arch Phys Med Rehabil. 2001 Nov;82(11):1520-5. doi: 10.1053/apmr.2001.25912. Arch Phys Med Rehabil. 2001. PMID: 11689970
-
Long-term follow-up of spinal cord stimulation to restore cough in subjects with spinal cord injury.J Spinal Cord Med. 2014 Jul;37(4):380-8. doi: 10.1179/2045772313Y.0000000152. Epub 2013 Nov 26. J Spinal Cord Med. 2014. PMID: 24090524 Free PMC article.
-
Restoration of respiratory muscle function following spinal cord injury. Review of electrical and magnetic stimulation techniques.Respir Physiol Neurobiol. 2005 Jul 28;147(2-3):273-87. doi: 10.1016/j.resp.2005.03.007. Respir Physiol Neurobiol. 2005. PMID: 16046197 Review.
-
Pulmonary function and spinal cord injury.Respir Physiol Neurobiol. 2009 May 15;166(3):129-41. doi: 10.1016/j.resp.2009.04.002. Epub 2009 Apr 9. Respir Physiol Neurobiol. 2009. PMID: 19442929 Review.
Cited by
-
Effects of Lower Thoracic Spinal Cord Stimulation on Bowel Management in Individuals With Spinal Cord Injury.Arch Phys Med Rehabil. 2021 Jun;102(6):1155-1164. doi: 10.1016/j.apmr.2020.09.394. Epub 2020 Nov 5. Arch Phys Med Rehabil. 2021. PMID: 33161007 Free PMC article. Clinical Trial.
-
Impact of the cough stimulation system on the care burden and life quality of caregivers of tetraplegics.J Spinal Cord Med. 2023 Sep;46(5):778-788. doi: 10.1080/10790268.2022.2148845. Epub 2023 Apr 5. J Spinal Cord Med. 2023. PMID: 37017634 Free PMC article.
-
Comparison of disc and wire electrodes to restore cough via lower thoracic spinal cord stimulation.J Spinal Cord Med. 2022 May;45(3):354-363. doi: 10.1080/10790268.2021.1936388. Epub 2021 Jul 7. J Spinal Cord Med. 2022. PMID: 34232841 Free PMC article. Clinical Trial.
-
Complete Restoration of Respiratory Muscle Function in Subjects With Spinal Cord Injury: Interventional Clinical Trial.Am J Phys Med Rehabil. 2020 Jul;99(7):e91-e92. doi: 10.1097/PHM.0000000000001338. Am J Phys Med Rehabil. 2020. PMID: 31688014 Free PMC article. No abstract available.
-
Effects of restoration of cough via spinal cord stimulation on subject quality of life.J Clin Orthop Trauma. 2022 Sep 27;34:102027. doi: 10.1016/j.jcot.2022.102027. eCollection 2022 Nov. J Clin Orthop Trauma. 2022. PMID: 36212771 Free PMC article.
References
-
- National Spinal Cord Injury Statistical Center , Facts and Figures at a Glance. Birmingham, AL: University of Alabama at Birmingham, 2015. https://www.nscisc.uab.edu/PublicDocuments/fact_figures_docs/Facts%20201.... Accessed August 18, 2016.
-
- Marsolais EB, Boninger ML, McCormick PC, . et al. Respiratory management following spinal cord injury: A clinical practice guideline for health-care professionals. J Spinal Cord Med. 2005; 28 3: 259– 293. - PubMed
-
- Meyers AR, Feltin M, Master RJ, . et al. Rehospitalization and spinal cord injury: Cross-sectional survey of adults living independently. Arch Phys Med Rehabil. 1985; 66 10: 704– 708. - PubMed
-
- Cardenas DD, Hoffman JM, Kirshblum S, McKinley W.. Etiology and incidence of rehospitalization after traumatic spinal cord injury: A multicenter analysis. Arch Phys Med Rehabil. 2004; 85 11: 1757– 1763. - PubMed
-
- Samsa GP, Landsman PB, Hamilton B.. Inpatient hospital utilization among veterans with traumatic spinal cord injury. Arch Phys Med Rehabil. 1996; 77 10: 1037– 1043. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical