

Concurrent brain radiotherapy and EGFR-TKI may improve intracranial metastases control in non-small cell lung cancer and have survival benefit in patients with low DS-GPA score
- PMID: 29340055
- PMCID: PMC5762323
- DOI: 10.18632/oncotarget.22785
Concurrent brain radiotherapy and EGFR-TKI may improve intracranial metastases control in non-small cell lung cancer and have survival benefit in patients with low DS-GPA score
Abstract
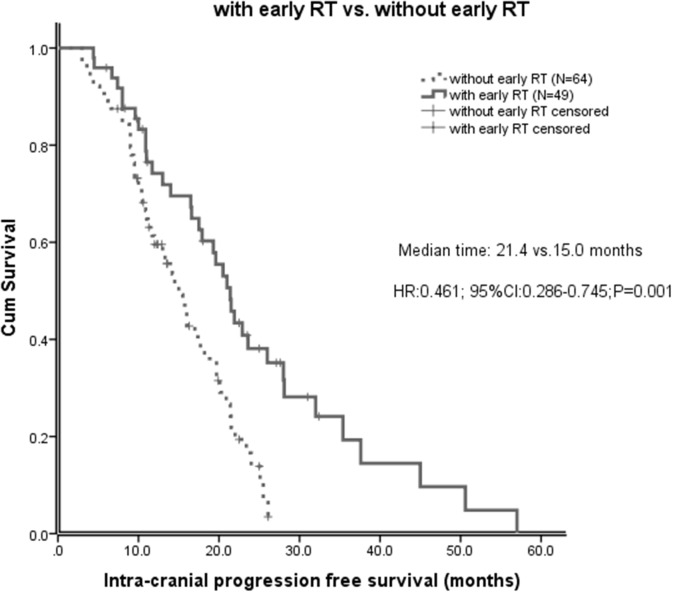
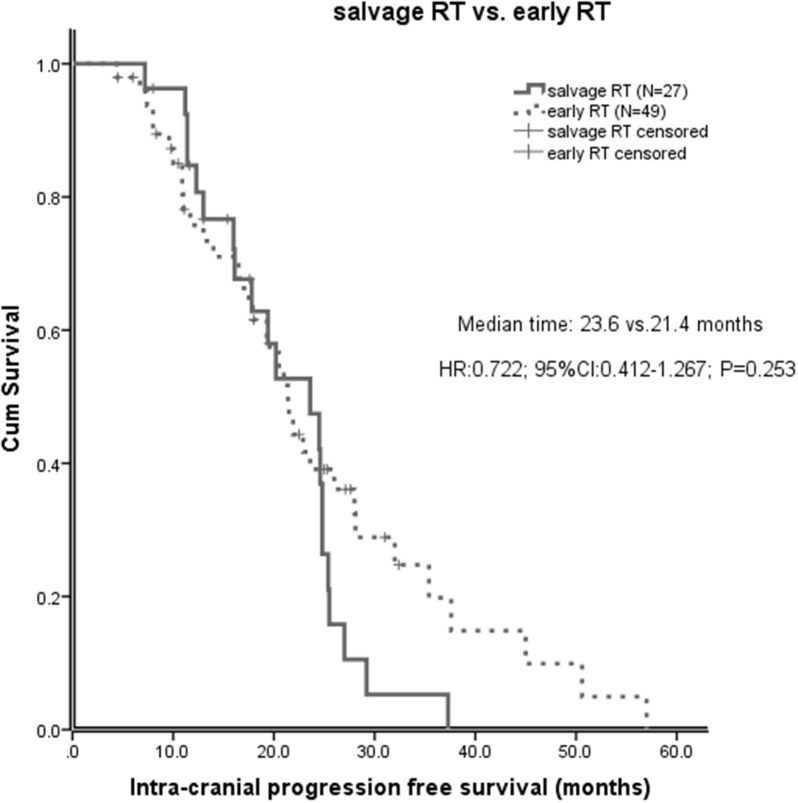
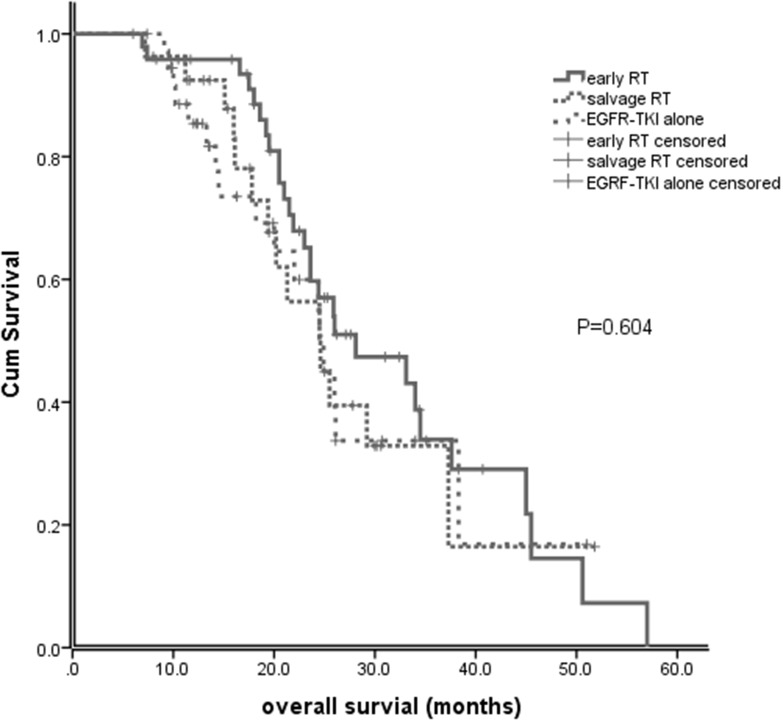
Epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) has intracranial activity in EGFR-mutant Non-Small Cell Lung Cancer (NSCLC). The optimal timing of brain radiotherapy (RT) and appropriate patients who need early brain RT remains undetermined. This is a retrospective study of EGFR-mutant NSCLC patients with newly diagnosed brain metastases (BMs) before EGFR-TKI initiation. Intra-cranial progression free survival (IC-PFS) and overall survival (OS) were measured from the date of EGFR-TKI treatment. A total of 113 patients were eligible, 49 received concurrent early brain RT with EGFR-TKI and 64 were treated with EGFR-TKI alone as initial therapy, including 27 with salvage RT upon BM progression. The patients with early brain RT had superior IC-PFS than those without early brain RT (21.4 vs 15.0 months, P=0.001), which remained significant in multivariate analysis (HR 0.30, P<0.001). The median overall survival (OS) for early RT, EGFR-TKI alone and salvage RT groups was 28.1, 24.5, and 24.6 months, respectively (P=0.604). Similar IC-PFS (23.6 vs 21.4 months, P=0.253) and OS (24.6 vs 28.1 months, P=0.385) were observed between salvage RT and early RT groups. For patients with Diagnosis-Specific Graded Prognostic Assessment (DS-GPA) score of 0 to 2, early brain RT was the independent factor for improved OS (HR 0.33, P=0.025). In conclusion, concurrent early brain RT with EGFR-TKI may improve intracranial disease control in EGFR-mutant NSCLC with BM and have survival benefit in patients with low DS-GPA score. Salvage brain RT upon BM progression may be acceptable in some patients.
Keywords: EGFR mutation; EGFR-TKI; brain metastasis; brain radiotherapy; non-small cell lung cancer.
Conflict of interest statement
CONFLICTS OF INTEREST All authors have declared no conflicts of interest.
Figures
References
-
- Berger LA, Riesenberg H, Bokemeyer C, Atanackovic D. CNS metastases in non-small-cell lung cancer: current role of EGFR-TKI therapy and future perspectives. Lung Cancer. 2013;80:242–248. - PubMed
-
- Shin DY, Na II, Kim CH, Park S, Baek H, Yang SH. EGFR mutation and brain metastasis in pulmonary adenocarcinomas. J Thorac Oncol. 2014;9:195–199. - PubMed
-
- Khuntia D, Brown P, Li J, Mehta MP. Whole-brain radiotherapy in the management of brain metastasis. J Clin Oncol. 2006;24:1295–1304. - PubMed
-
- Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, Sneed PK, Chao ST, Weil RJ, Suh J, Bhatt A, Jensen AW, Brown PD, et al. Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. 2012;30:419–425. - PMC - PubMed
-
- Sperduto PW, Yang TJ, Beal K, Pan H, Brown PD, Bangdiwala A, Shanley R, Yeh N, Gaspar LE, Braunstein S, Sneed P, Boyle J, Kirkpatrick JP, et al. Estimating survival in patients with lung cancer and brain metastases: an update of the graded prognostic assessment for lung cancer using molecular markers (Lung-molGPA) JAMA Oncol. 2016 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
