

Treatment of Severe Hyperkalemia: Confronting 4 Fallacies
- PMID: 29340313
- PMCID: PMC5762976
- DOI: 10.1016/j.ekir.2017.10.001
Treatment of Severe Hyperkalemia: Confronting 4 Fallacies
Abstract
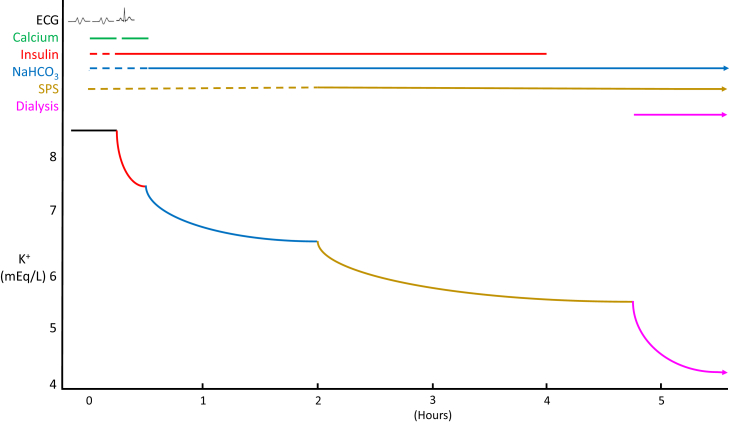
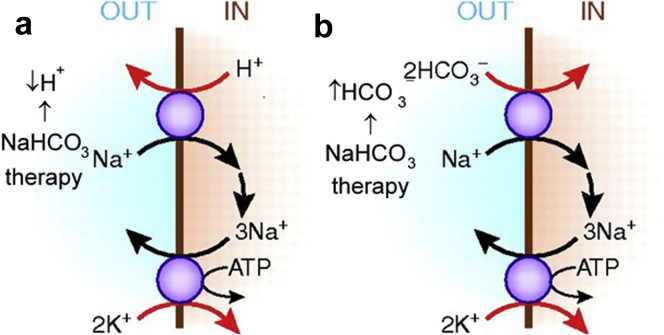
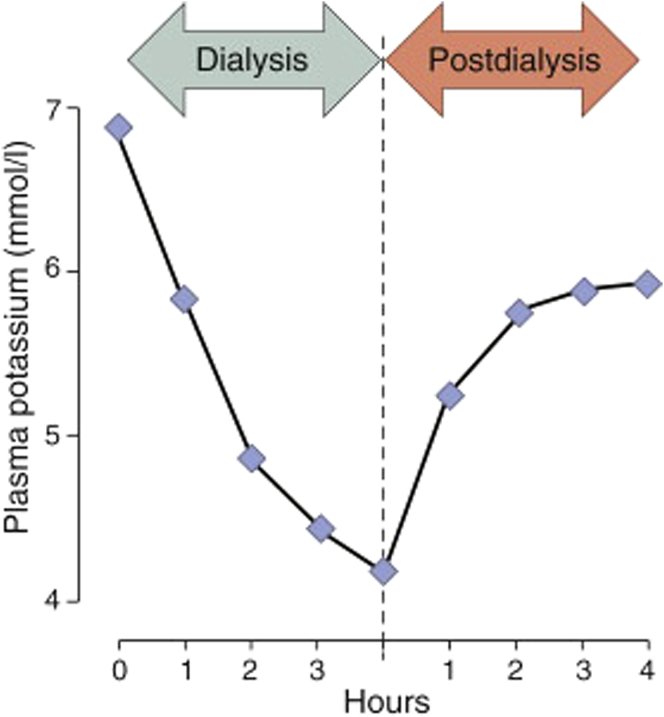
Severe hyperkalemia is a medical emergency that can cause lethal arrhythmias. Successful management requires monitoring of the electrocardiogram and serum potassium concentrations, the prompt institution of therapies that work both synergistically and sequentially, and timely repeat dosing as necessary. It is of concern then that, based on questions about effectiveness and safety, many physicians no longer use 3 key modalities in the treatment of severe hyperkalemia: sodium bicarbonate, sodium polystyrene sulfonate (Kayexalate [Concordia Pharmaceuticals Inc., Oakville, ON, Canada], SPS [CMP Pharma, Farmville, NC]), and hemodialysis with low potassium dialysate. After reviewing older reports and newer information, I believe that these exclusions are ill advised. In this article, I briefly discuss the treatment of severe hyperkalemia and detail why these modalities are safe and effective and merit inclusion in the treatment of severe hyperkalemia.
Keywords: Kayexalate; colonic necrosis; low potassium dialysate; severe hyperkalemia; sodium bicarbonate; sodium polystyrene sulfonate.
Figures
References
-
- Acker C.G., Johnson J.P., Palevsky P.M. Hyperkalemia in hospitalized patients. Arch Intern Med. 1998;158:917–924. - PubMed
-
- Muschart X., Boulouffe C., Jamart J. A determination of the current causes of hyperkalaemia and whether they have changed over the past 25 years. Acta Clinica Belgica. 2014;69:280–284. - PubMed
-
- Hagan A.E., Farrington C.A., Wall G.C. Sodium polystyrene sulfonate for the treatment of acute hyperkalemia: a retrospective study. Clin Nephrol. 2015;85:38–43. - PubMed
-
- Mount D.B. Disorders of potassium balance. In: Skorecki K., Chertow G.M., Marsden P.A., Taal M.W., Wasser W.G., editors. Brenner and Rector’s The Kidney. 10th ed. Elsevier; Philadelphia: 2016. pp. 559–600.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
