

Nephrin Loss Can Be Used to Predict Remission and Long-term Renal Outcome in Patients With Minimal Change Disease
- PMID: 29340328
- PMCID: PMC5762955
- DOI: 10.1016/j.ekir.2017.09.011
Nephrin Loss Can Be Used to Predict Remission and Long-term Renal Outcome in Patients With Minimal Change Disease
Abstract
Introduction: Minimal change disease is a common cause of nephrotic syndrome. In general, patients with minimal change disease respond to corticosteroids and have excellent long-term renal survival. However, some patients have less favorable outcome. These patients are often thought to have progressed to focal segmental glomerulosclerosis. We previously reported that a segmental loss of podocyte markers is present before the development of focal segmental glomerulosclerosis in a rat model. Here, we investigated whether loss of podocyte marker nephrin can serve as a biomarker for predicting poor outcome in patients with minimal change disease.
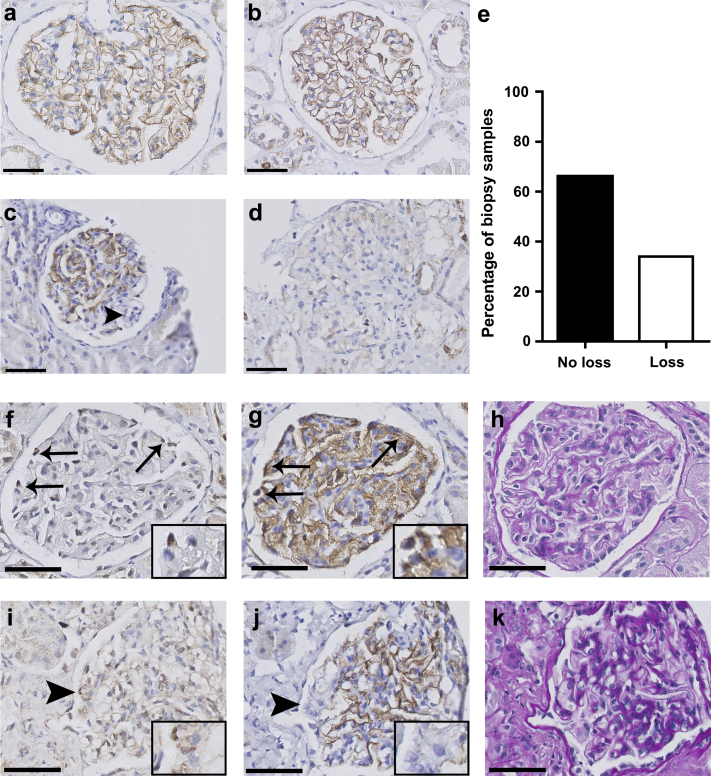
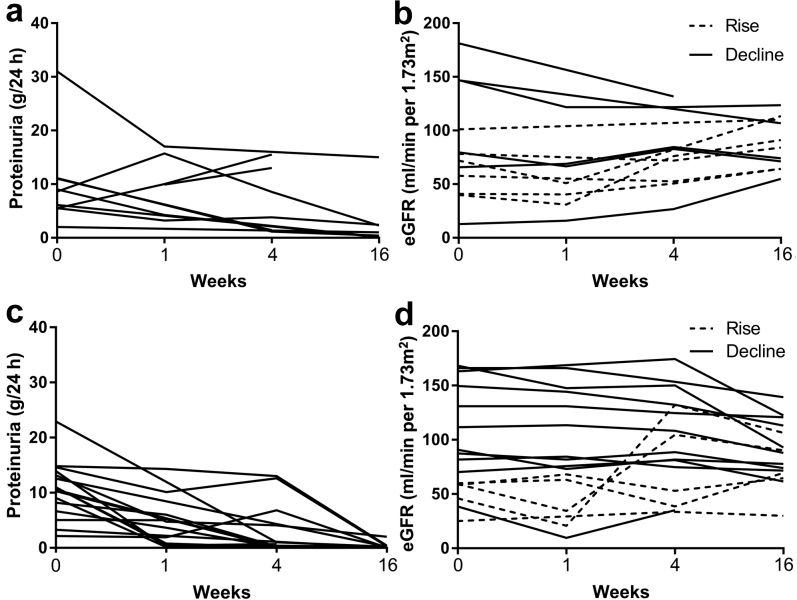
Methods: We obtained 47 kidney biopsy samples from patients diagnosed with minimal change disease and stained sections with periodic acid-Schiff and for nephrin. Nephrin loss was scored by 2 independent researchers who were blinded to clinical outcome. Clinical data were collected retrospectively, and nephrin loss was correlated with clinical follow-up data.
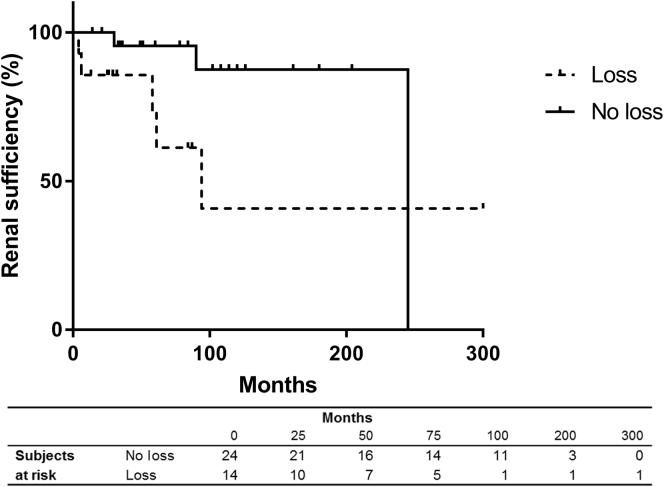
Results: Nephrin loss was present in 34% of the biopsy samples. During follow-up, patients with nephrin loss achieved remission less frequently (61%) compared to patients without (96%) (P = 0.002). Moreover, 5-year eGFR was lower in the patients with renal nephrin loss. The risk of eGFR decreasing to < 60 ml/min per 1.73m2 increased with each percentage of glomeruli with nephrin loss (hazard ratio = 1.044, 95% confidence interval = 1.02-1.07).
Conclusion: These results indicate that nephrin loss in patients with minimal change disease can help predict both remission and long-term renal outcome.
Keywords: biomarker; focal segmental glomerulosclerosis; minimal change disease; nephrin; nephrotic syndrome.
Figures
References
-
- Fogo A.B. Minimal change disease and focal segmental glomerulosclerosis. Nephrol Dial Transplant. 2001;16(suppl 6):74–76. - PubMed
-
- Chembo C.L., Marshall M.R., Williams L.C. Long-term outcomes for primary glomerulonephritis: New Zealand Glomerulonephritis Study. Nephrology [Carlton] 2015;20:899–907. - PubMed
-
- Nolasco F., Cameron J.S., Heywood E.F. Adult-onset minimal change nephrotic syndrome: a long-term follow-up. Kidney Int. 1986;29:1215–1223. - PubMed
-
- Idelson B.A., Smithline N., Smith G.W. Prognosis in steroid-treated idiopathic nephrotic syndrome in adults. Analysis of major predictive factors after ten-year follow-up. Arch Intern Med. 1977;137:891–896. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
