

HEPATOCELLULAR CARCINOMA: DIAGNOSIS AND OPERATIVE MANAGEMENT
- PMID: 29340553
- PMCID: PMC5793147
- DOI: 10.1590/0102-6720201700040011
HEPATOCELLULAR CARCINOMA: DIAGNOSIS AND OPERATIVE MANAGEMENT
Abstract
Introduction: Hepatocellular carcinoma is an aggressive malignant tumor with high lethality.
Aim: To review diagnosis and management of hepatocellular carcinoma.
Methods: Literature review using web databases Medline/PubMed.
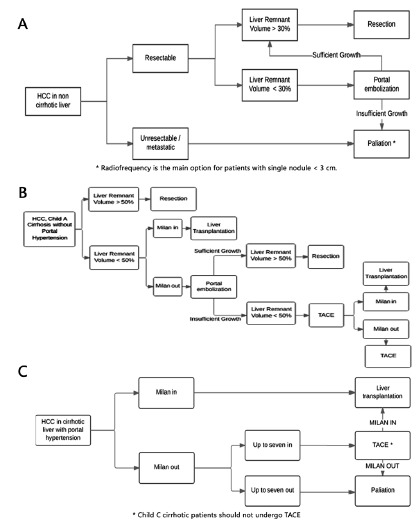
Results: Hepatocellular carcinoma is a common complication of hepatic cirrhosis. Chronic viral hepatitis B and C also constitute as risk factors for its development. In patients with cirrhosis, hepatocelular carcinoma usually rises upon malignant transformation of a dysplastic regenerative nodule. Differential diagnosis with other liver tumors is obtained through computed tomography scan with intravenous contrast. Magnetic resonance may be helpful in some instances. The only potentially curative treatment for hepatocellular carcinoma is tumor resection, which may be performed through partial liver resection or liver transplantation. Only 15% of all hepatocellular carcinomas are amenable to operative treatment. Patients with Child C liver cirrhosis are not amenable to partial liver resections. The only curative treatment for hepatocellular carcinomas in patients with Child C cirrhosis is liver transplantation. In most countries, only patients with hepatocellular carcinoma under Milan Criteria are considered candidates to a liver transplant.
Conclusion: Hepatocellular carcinoma is potentially curable if discovered in its initial stages. Medical staff should be familiar with strategies for early diagnosis and treatment of hepatocellular carcinoma as a way to decrease mortality associated with this malignant neoplasm.
O carcinoma hepatocelular é neoplasia maligna agressiva com elevada morbidade e mortalidade.
Revisão sobre a fisiopatologia, o diagnóstico e o manejo do carcinoma hepatocelular nos vários estágios da doença.
Revisão da literatura utilizando a base Medline/PubMed e literatura adicional.
O carcinoma hepatocelular é geralmente complicação da cirrose hepática. As hepatites virais crônicas B e C também são fatores de risco para o surgimento do carcinoma hepatocelular. Quando associado à cirrose hepática, ele geralmente surge a partir da evolução de um nódulo regenerativo hepatocitário que sofre degeneração maligna. O diagnóstico é efetuado através de tomografia computadorizada de abdome com contraste endovenoso, e a ressonância magnética pode auxiliar nos casos que não possam ser definidos pela tomografia. O único tratamento potencialmente curativo para o carcinoma hepatocelular é a ressecção do tumor, seja ela realizada através de hepatectomia parcial ou de transplante. Infelizmente, apenas cerca de 15% dos carcinomas hepatocelulares são passíveis de tratamento cirúrgico. Pacientes portadores de cirrose hepática estágio Child B e C não devem ser submetidos à ressecção hepática parcial. Para esses pacientes, as opções terapêuticas curativas restringem-se ao transplante de fígado, desde que selecionáveis para esse procedimento, o que na maioria dos países dá-se através dos Critérios de Milão.
Quando diagnosticado em seus estágios iniciais, o carcinoma hepatocelular é potencialmente curável. O melhor conhecimento das estratégias de diagnóstico e tratamento propiciam sua identificação precoce e a indicação de tratamento apropriado.
Conflict of interest statement
Figures
References
-
- Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) tips and tricks. J Gastrointest Surg. 2013;17:814–821. - PubMed
-
- Bismuth H, Chiche L. Surgery of hepatic tumors. Prog. Liver Dis. 1993;11:279e295–279e295. - PubMed
-
- Bruix J, Reig M, Sherman M. Evidence-Based Diagnosis, Staging, and Treatment of Patients With Hepatocellular Carcinoma. Gastroenterology. 2016;150:835–853. - PubMed
-
- Bruix J, Takayama T, Mazzaferro V. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM) a phase 3, randomised, double blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
