

Antimicrobial-Resistant Klebsiella pneumoniae Carriage and Infection in Specialized Geriatric Care Wards Linked to Acquisition in the Referring Hospital
- PMID: 29340588
- PMCID: PMC6030810
- DOI: 10.1093/cid/ciy027
Antimicrobial-Resistant Klebsiella pneumoniae Carriage and Infection in Specialized Geriatric Care Wards Linked to Acquisition in the Referring Hospital
Abstract
Background: Klebsiella pneumoniae is a leading cause of extended-spectrum β-lactamase (ESBL)-producing hospital-associated infections, for which elderly patients are at increased risk.
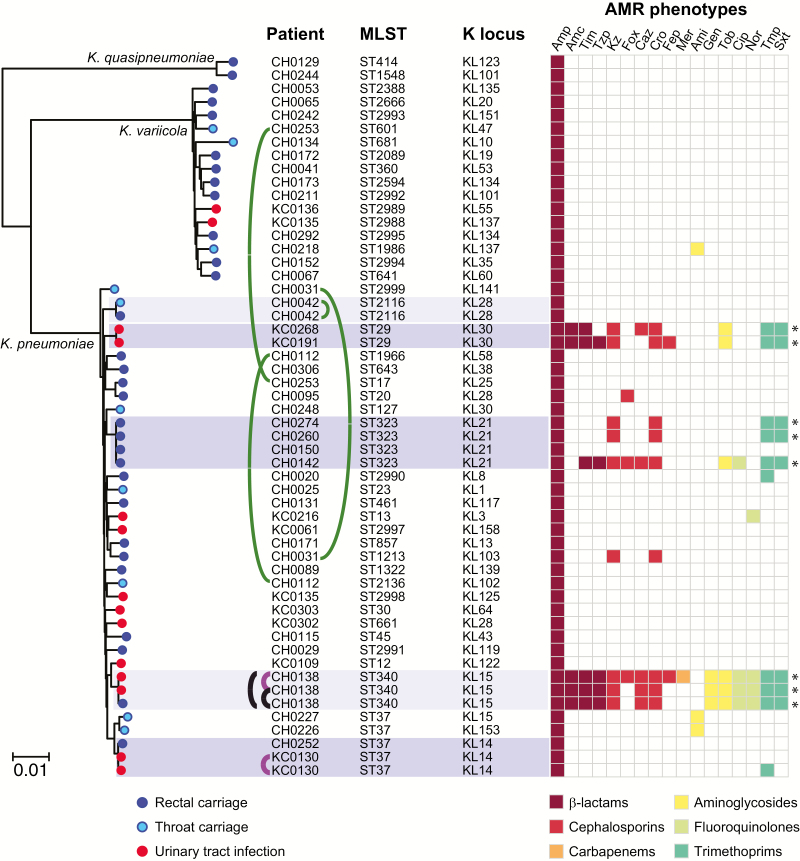
Methods: We conducted a 1-year prospective cohort study, in which a third of patients admitted to 2 geriatric wards in a specialized hospital were recruited and screened for carriage of K. pneumoniae by microbiological culture. Clinical isolates were monitored via the hospital laboratory. Colonizing and clinical isolates were subjected to whole-genome sequencing and antimicrobial susceptibility testing.
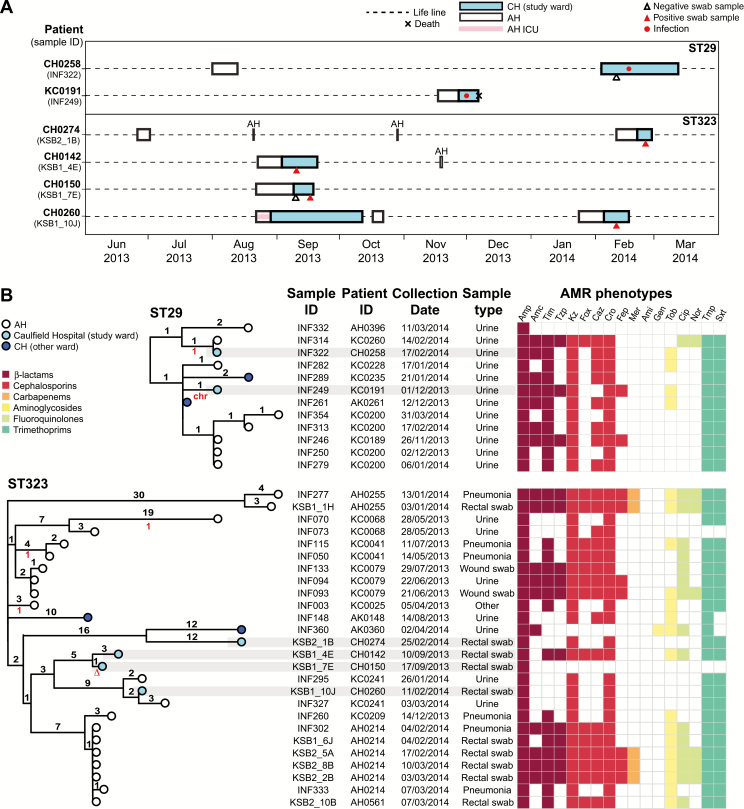
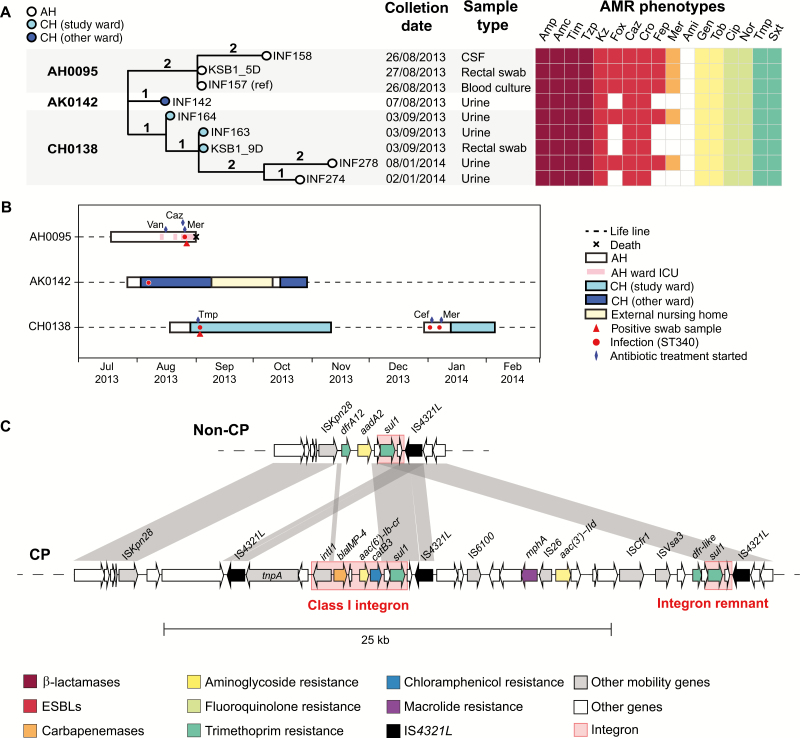
Results: K. pneumoniae throat carriage prevalence was 4.1%, rectal carriage 10.8%, and ESBL carriage 1.7%, and the incidence of K. pneumoniae infection was 1.2%. The isolates were diverse, and most patients were colonized or infected with a unique phylogenetic lineage, with no evidence of transmission in the wards. ESBL strains carried blaCTX-M-15 and belonged to clones associated with hospital-acquired ESBL infections in other countries (sequence type [ST] 29, ST323, and ST340). One also carried the carbapenemase blaIMP-26. Genomic and epidemiological data provided evidence that ESBL strains were acquired in the referring hospital. Nanopore sequencing also identified strain-to-strain transmission of a blaCTX-M-15 FIBK/FIIK plasmid in the referring hospital.
Conclusions: The data suggest the major source of K. pneumoniae was the patient's own gut microbiome, but ESBL strains were acquired in the referring hospital. This highlights the importance of the wider hospital network to understanding K. pneumoniae risk and infection prevention. Rectal screening for ESBL organisms on admission to geriatric wards could help inform patient management and infection control in such facilities.
Figures
References
-
- Pendleton JN, Gorman SP, Gilmore BF. Clinical relevance of the ESKAPE pathogens. Expert Rev Anti Infect Ther 2013; 11:297–308. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
