

Association of Bariatric Surgery vs Medical Obesity Treatment With Long-term Medical Complications and Obesity-Related Comorbidities
- PMID: 29340680
- PMCID: PMC5833560
- DOI: 10.1001/jama.2017.21055
Association of Bariatric Surgery vs Medical Obesity Treatment With Long-term Medical Complications and Obesity-Related Comorbidities
Abstract
Importance: The association of bariatric surgery and specialized medical obesity treatment with beneficial and detrimental outcomes remains uncertain.
Objective: To compare changes in obesity-related comorbidities in patients with severe obesity (body mass index ≥40 or ≥35 and at least 1 comorbidity) undergoing bariatric surgery or specialized medical treatment.
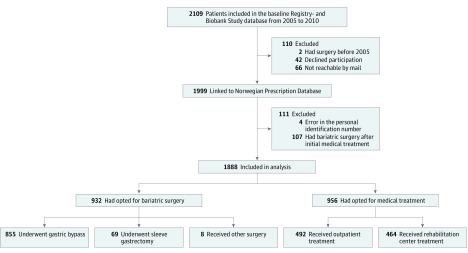
Design, setting, and participants: Cohort study with baseline data of exposures from November 2005 through July 2010 and follow-up data from 2006 until death or through December 2015 at a tertiary care outpatient center, Vestfold Hospital Trust, Norway. Consecutive treatment-seeking adult patients (n = 2109) with severe obesity assessed (221 patients excluded and 1888 patients included).
Exposures: Bariatric surgery (n = 932, 92% gastric bypass) or specialized medical treatment (n = 956) including individual or group-based lifestyle intervention programs.
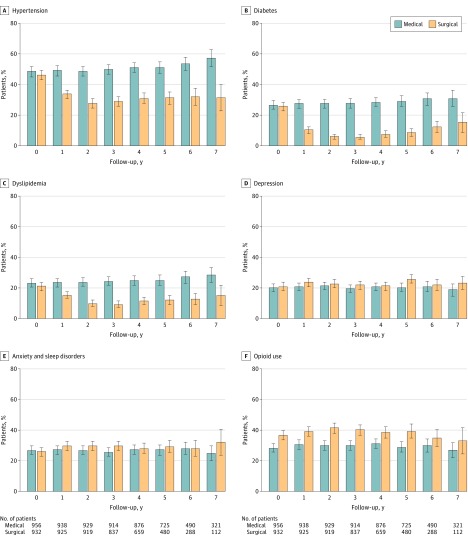
Main outcomes and measures: Primary outcomes included remission and new onset of hypertension based on drugs dispensed according to the Norwegian Prescription Database. Prespecified secondary outcomes included changes in comorbidities. Adverse events included complications retrieved from the Norwegian Patient Registry and a local laboratory database.
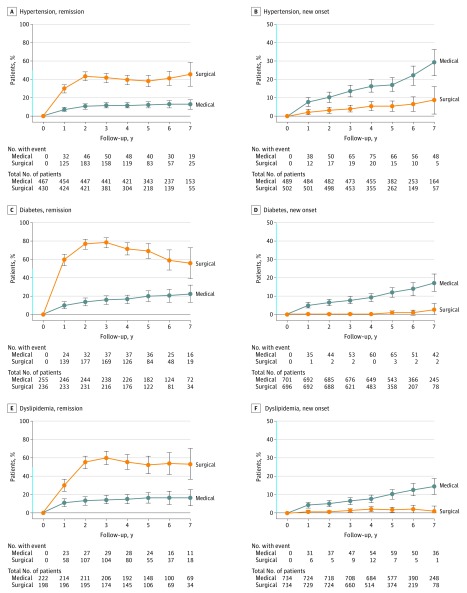
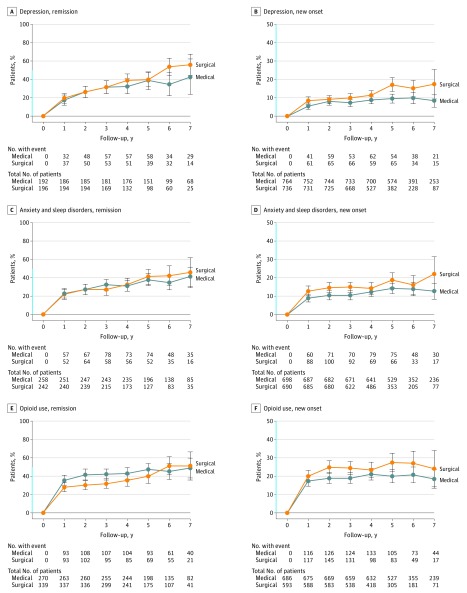
Results: Among 1888 patients included in the study, the mean (SD) age was 43.5 (12.3) years (1249 women [66%]; mean [SD] baseline BMI, 44.2 [6.1]; 100% completed follow-up at a median of 6.5 years [range, 0.2-10.1]). Surgically treated patients had a greater likelihood of remission and lesser likelihood for new onset of hypertension (remission: absolute risk [AR], 31.9% vs 12.4%); risk difference [RD], 19.5% [95% CI, 15.8%-23.2%], relative risk [RR], 2.1 [95% CI, 2.0-2.2]; new onset: AR, 3.5% vs 12.2%, RD, 8.7% [95% CI, 6.7%-10.7%], RR, 0.4 [95% CI, 0.3-0.5]; greater likelihood of diabetes remission: AR, 57.5% vs 14.8%; RD, 42.7% [95% CI, 35.8%-49.7%], RR, 3.9 [95% CI, 2.8-5.4]; greater risk of new-onset depression: AR, 8.9% vs 6.5%; RD, 2.4% [95% CI, 1.3%-3.5%], RR, 1.5 [95% CI, 1.4-1.7]; and treatment with opioids: AR, 19.4% vs 15.8%, RD, 3.6% [95% CI, 2.3%-4.9%], RR, 1.3 [95% CI, 1.2-1.4]). Surgical patients had a greater risk for undergoing at least 1 additional gastrointestinal surgical procedure (AR, 31.3% vs 15.5%; RD, 15.8% [95% CI, 13.1%-18.5%]; RR, 2.0 [95% CI, 1.7-2.4]). The proportion of patients with low ferritin levels was significantly greater in the surgical group (26% vs 12%, P < .001).
Conclusions and relevance: Among patients with severe obesity followed up for a median of 6.5 years, bariatric surgery compared with medical treatment was associated with a clinically important increased risk for complications, as well as lower risks of obesity-related comorbidities. The risk for complications should be considered in the decision-making process.
Conflict of interest statement
Figures
Comment in
-
Reimagining Obesity in 2018: A JAMA Theme Issue on Obesity.JAMA. 2018 Jan 16;319(3):238-240. doi: 10.1001/jama.2017.21779. JAMA. 2018. PMID: 29340660 No abstract available.
References
-
- World Health Organization Obesity and overweight. http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed June 25, 2017.
-
- Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164(2):328-334. - PubMed
-
- Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. 2017;376(3):254-266. - PubMed
-
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013 Executive summary: guidelines (2013) for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines: based on a systematic review from the Obesity Expert Panel, 2013. Obesity (Silver Spring). 2014;22(suppl 2):S5-S39. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
