

Differentiation of glioblastoma multiforme, metastases and primary central nervous system lymphomas using multiparametric perfusion and diffusion MR imaging of a tumor core and a peritumoral zone-Searching for a practical approach
- PMID: 29342201
- PMCID: PMC5771619
- DOI: 10.1371/journal.pone.0191341
Differentiation of glioblastoma multiforme, metastases and primary central nervous system lymphomas using multiparametric perfusion and diffusion MR imaging of a tumor core and a peritumoral zone-Searching for a practical approach
Abstract
Introduction: In conventional MR examinations glioblastomas multiforme (GBMs), metastases and primary CNS lymphomas (PCNSLs) may show very similar appearance. The aim of the study was to evaluate usefulness of multiparametric T2*DSC perfusion and diffusion MR imaging in the preoperative differentiation of these tumors.
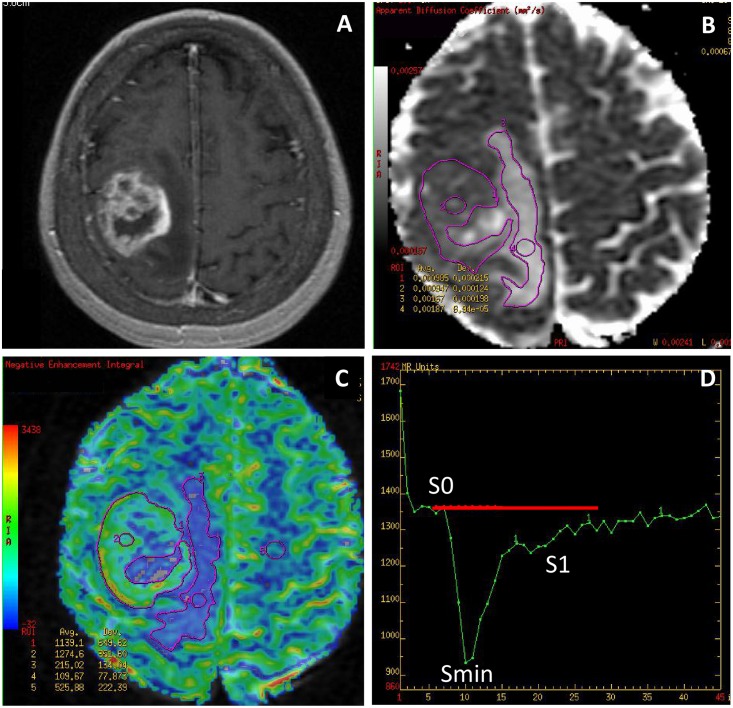
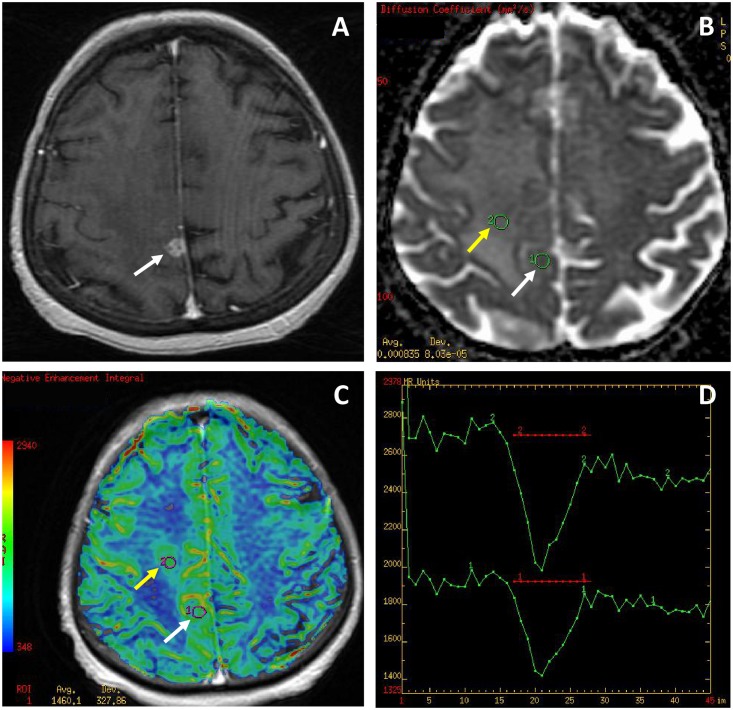
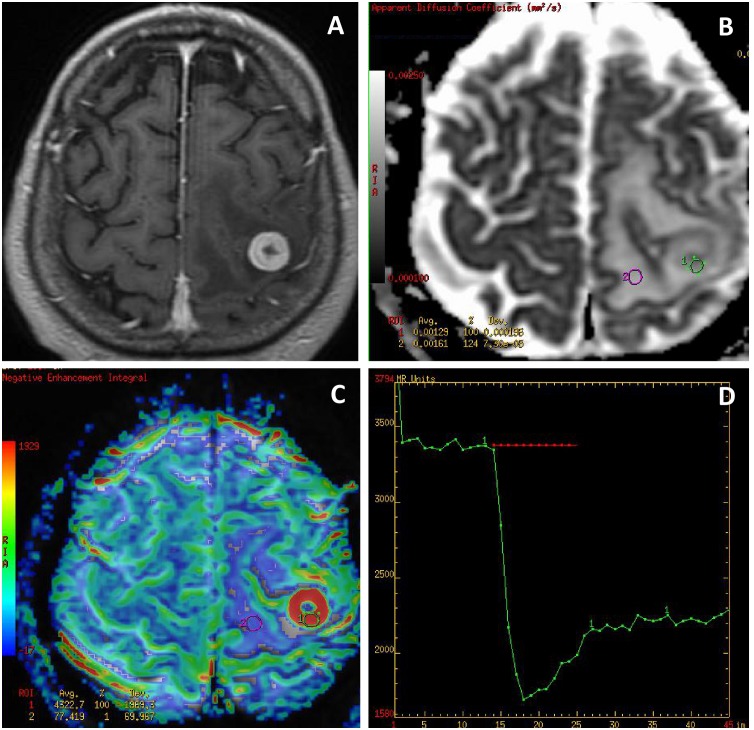
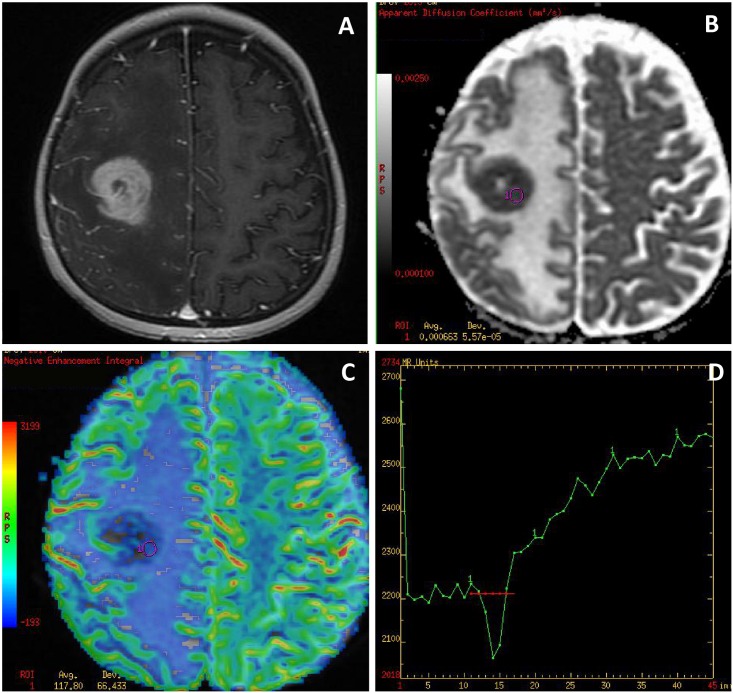
Material and methods: Seventy four solitary enhancing tumors (27 GBMs, 30 metastases, 17 PCNSLs) were enrolled in the study. Parameters of cerebral blood volume (rCBV), peak height (rPH), percentage of signal recovery (rPSR) and apparent diffusion coefficient (ADC) were assessed from the tumor core and the peritumoral non-enhancing T2-hyperintense zone.
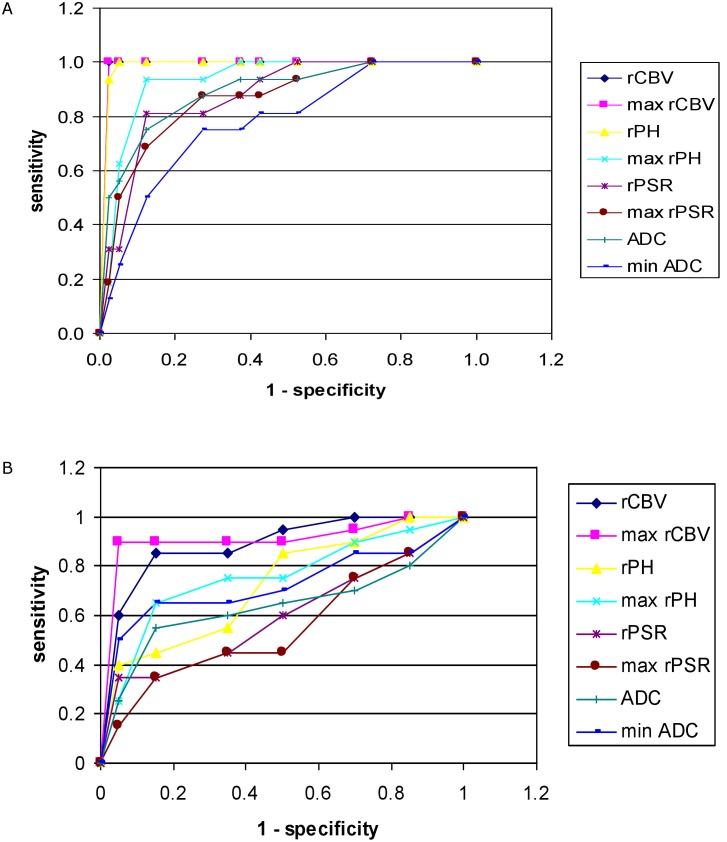
Results: Within the tumor core there were no differences in perfusion and diffusion parameters between GBMs and metastases. Compared to GBMs and metastases, PCNSLs showed significantly lower rCBV and rPH, ADC as well as higher rPSR values. Max rCBV with a cut-off value of 2.18 demonstrated the highest accuracy of 0.98 in differentiating PCNSLs from other tumors. To distinguish GBMs from metastases analysis of the peritumoral zone was performed showing significantly higher rCBV, rPH and lower ADC values in GBMs with the highest accuracy of 0.94 found for max rCBV at a cut-off value of 0.98.
Conclusions: Max rCBV seems to be the most important parameter to differentiate GBMs, metastases and PCNSLs. Analysis of max rCBV within the tumor core enables to distinguish hypoperfused PCNSLs from hyperperfused GBMs and metastases while evaluation of max rCBV within the peritumoral zone is helpful to distinguish GBMs showing peritumoral infiltration from metastases surrounded by pure edema.
Conflict of interest statement
Figures
References
-
- Omuro A, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013;310:1842–1850. doi: 10.1001/jama.2013.280319 - DOI - PubMed
-
- Sperduto PW, Chao ST, Sneed PK, Luo X, Suh J, Roberge D, et al. Diagnosis-specific prognostic factors, indexes, and treatment outcomes for patients with newly diagnosed brain metastases: a multi-institutional analysis of 4,259 patients. Int J Radiat Oncol Biol Phys. 2010;77:655–661. doi: 10.1016/j.ijrobp.2009.08.025 - DOI - PubMed
-
- Pasricha S, Gupta A, Gawande J, Trivedi P, Patel D. Primary central nervous system lymphoma: a study of clinicopathological features and trend in western India. Indian J Cancer. 2011;48:199–203. doi: 10.4103/0019-509X.82890 - DOI - PubMed
-
- Sugahara T, Korogi Y, Kochi M, Ikushima I, Shigematu Y, Hirai T, et al. Usefulness of diffusion-weighted MRI with echo-planar technique in the evaluation of cellularity in gliomas. J Magn Reson Imaging. 1999;9:53–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
