

Advancing Our Understanding of Protective Maternal Immunity as a Guide for Development of Vaccines To Reduce Congenital Cytomegalovirus Infections
- PMID: 29343580
- PMCID: PMC5972872
- DOI: 10.1128/JVI.00030-18
Advancing Our Understanding of Protective Maternal Immunity as a Guide for Development of Vaccines To Reduce Congenital Cytomegalovirus Infections
Abstract
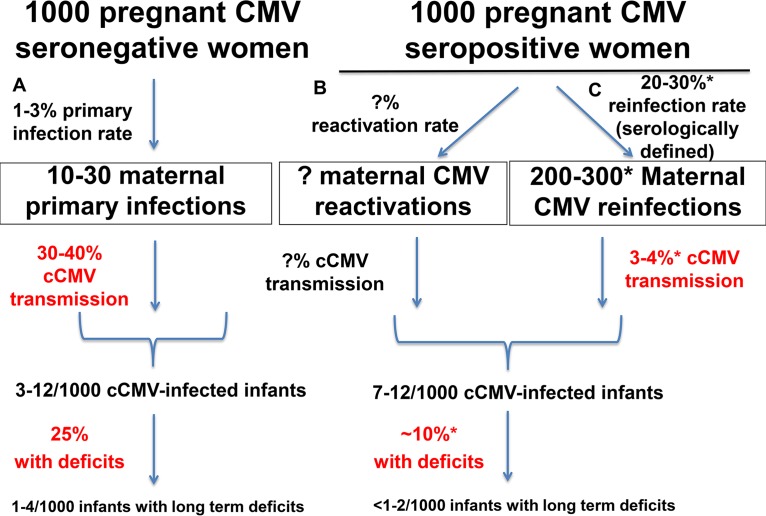
Human cytomegalovirus (HCMV) is the most common congenitally transmitted pathogen worldwide, impacting an estimated 1 million newborns annually. Congenital HCMV (cCMV) infection is a major global contributor to long-term neurologic deficits, including deafness, microcephaly, and neurodevelopmental delay, as well as to fetal loss and occasional infant mortality. Accordingly, design of a maternal vaccine to prevent cCMV continues to be a top public health priority. Nevertheless, we remain without a licensed vaccine. Maternal immunity provides partial protection, as the risk of vertical HCMV transmission from chronically infected mothers is reduced compared to settings in which the mother is newly infected during pregnancy. Therefore, an understanding of the maternal immune correlates of protection against cCMV is critical to informing design of an efficacious maternal vaccine. Although vaccine development is being assiduously pursued by a large number of pharmaceutical manufacturers, biotechnology organizations, and academic researchers, some pessimism has been expressed regarding the issue of whether a vaccine to protect against cCMV is possible. This pessimism is based on observations that natural immunity is not completely protective against maternal reinfection and congenital transmission. However, we assert that optimism regarding vaccine development is indeed justified, on the basis of accruing evidence of immune correlates of protection-readily achievable by vaccination-that are associated with reduced transmission of HCMV to the fetus in seronegative women. In light of the substantial burden on society conferred by cCMV infection, even a modest reduction in the occurrence of this fetal disease is an important public health goal and justifies aggressive clinical evaluation of vaccines currently in the pipeline.
Keywords: congenital infections; cytomegalovirus; vaccines.
Copyright © 2018 American Society for Microbiology.
Figures
Comment in
-
Higher Expectations for a Vaccine To Prevent Congenital Cytomegalovirus Infection.J Virol. 2018 Jul 17;92(15):e00764-18. doi: 10.1128/JVI.00764-18. Print 2018 Aug 1. J Virol. 2018. PMID: 30018143 Free PMC article. No abstract available.
-
Reply to Gantt et al., "Higher Expectations for a Vaccine To Prevent Congenital Cytomegalovirus Infection".J Virol. 2018 Jul 17;92(15):e00771-18. doi: 10.1128/JVI.00771-18. Print 2018 Aug 1. J Virol. 2018. PMID: 30018144 Free PMC article. No abstract available.
References
-
- Francis SS, Wallace AD, Wendt GA, Li L, Liu F, Riley LW, Kogan S, Walsh KM, de Smith AJ, Dahl GV, Ma X, Delwart E, Metayer C, Wiemels JL. 2017. In utero cytomegalovirus infection and development of childhood acute lymphoblastic leukemia. Blood 129:1680–1684. doi:10.1182/blood-2016-07-723148. - DOI - PMC - PubMed
-
- Stratton KR, Durch JS, Lawrence RS (ed). 2000. Vaccines for the 21st century: a tool for decisionmaking. National Academies Press, Washington, DC. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
