Hydrogel biomaterials and their therapeutic potential for muscle injuries and muscular dystrophies
- PMID: 29343633
- PMCID: PMC5805959
- DOI: 10.1098/rsif.2017.0380
Hydrogel biomaterials and their therapeutic potential for muscle injuries and muscular dystrophies
Abstract
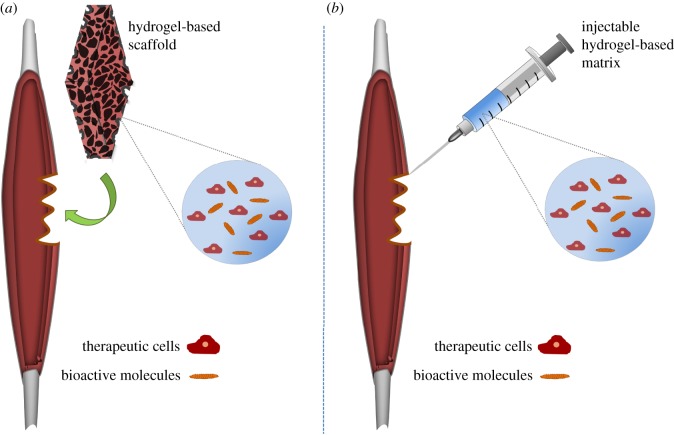
Muscular diseases such as muscular dystrophies and muscle injuries constitute a large group of ailments that manifest as muscle weakness, atrophy or fibrosis. Although cell therapy is a promising treatment option, the delivery and retention of cells in the muscle is difficult and prevents sustained regeneration needed for adequate functional improvements. Various types of biomaterials with different physical and chemical properties have been developed to improve the delivery of cells and/or growth factors for treating muscle injuries. Hydrogels are a family of materials with distinct advantages for use as cell delivery systems in muscle injuries and ailments, including their mild processing conditions, their similarities to natural tissue extracellular matrix, and their ability to be delivered with less invasive approaches. Moreover, hydrogels can be made to completely degrade in the body, leaving behind their biological payload in a process that can enhance the therapeutic process. For these reasons, hydrogels have shown great potential as cell delivery matrices. This paper reviews a few of the hydrogel systems currently being applied together with cell therapy and/or growth factor delivery to promote the therapeutic repair of muscle injuries and muscle wasting diseases such as muscular dystrophies.
Keywords: biomaterials; growth factors; muscle cells; scaffolds; tissue engineering.
© 2018 The Author(s).
Conflict of interest statement
We declare we have no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical