

HumanMethylation450K Array-Identified Biomarkers Predict Tumour Recurrence/Progression at Initial Diagnosis of High-risk Non-muscle Invasive Bladder Cancer
- PMID: 29343995
- PMCID: PMC5764140
- DOI: 10.1177/1179299X17751920
HumanMethylation450K Array-Identified Biomarkers Predict Tumour Recurrence/Progression at Initial Diagnosis of High-risk Non-muscle Invasive Bladder Cancer
Abstract
Background: High-risk non-muscle invasive bladder cancer (HR-NMIBC) is a clinically unpredictable disease. Despite clinical risk estimation tools, many patients are undertreated with intra-vesical therapies alone, whereas others may be over-treated with early radical surgery. Molecular biomarkers, particularly DNA methylation, have been reported as predictive of tumour/patient outcomes in numerous solid organ and haematologic malignancies; however, there are few reports in HR-NMIBC and none using genome-wide array assessment. We therefore sought to identify novel DNA methylation markers of HR-NMIBC clinical outcomes that might predict tumour behaviour at initial diagnosis and help guide patient management.
Patients and methods: A total of 21 primary initial diagnosis HR-NMIBC tumours were analysed by Illumina HumanMethylation450 BeadChip arrays and subsequently bisulphite Pyrosequencing. In all, 7 had not recurred at 1 year after resection and 14 had recurred and/or progressed despite intra-vesical BCG. A further independent cohort of 32 HR-NMIBC tumours (17 no recurrence and 15 recurrence and/or progression despite BCG) were also assessed by bisulphite Pyrosequencing.
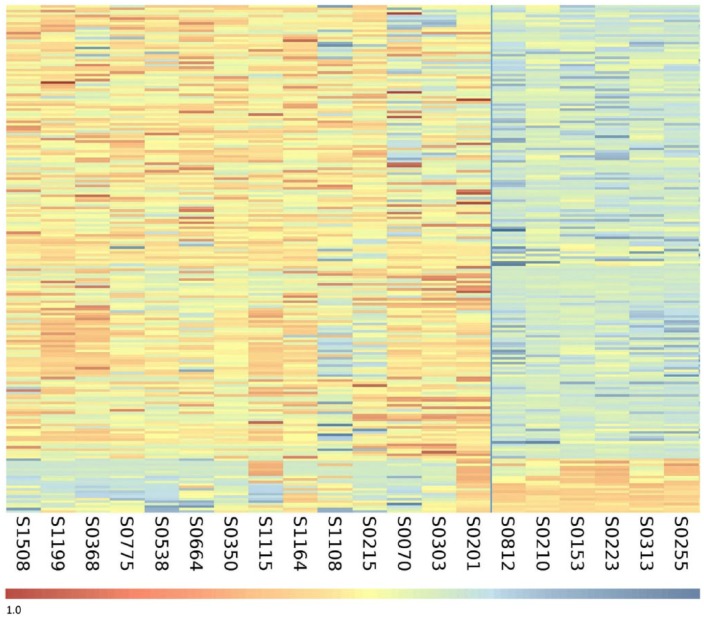
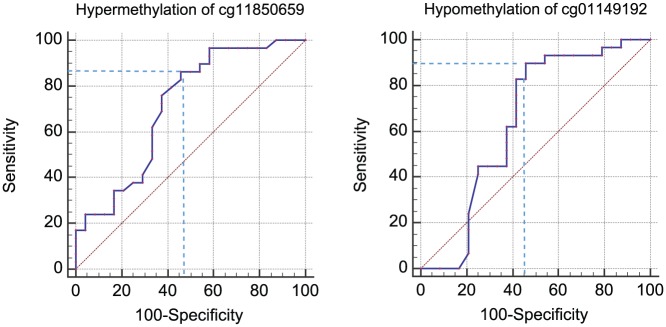
Results: Array analyses identified 206 CpG loci that segregated non-recurrent HR-NMIBC tumours from clinically more aggressive recurrence/progression tumours. Hypermethylation of CpG cg11850659 and hypomethylation of CpG cg01149192 in combination predicted HR-NMIBC recurrence and/or progression within 1 year of diagnosis with 83% sensitivity, 79% specificity, and 83% positive and 79% negative predictive values.
Conclusions: This is the first genome-wide DNA methylation analysis of a unique HR-NMIBC tumour cohort encompassing known 1-year clinical outcomes. Our analyses identified potential novel epigenetic markers that could help guide individual patient management in this clinically unpredictable disease.
Keywords: HumanMethylation450 BeadChip array; epigenetics; high-risk non-muscle invasive bladder cancer; methylation; prognostic biomarker.
Conflict of interest statement
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E366. - PubMed
-
- Kirkali Z, Chan T, Manoharan M, et al. Bladder cancer: epidemiology, staging and grading, and diagnosis. Urology. 2005;66:4–34. - PubMed
-
- Sylvester RJ, van der Meijden AP, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49:466–475 (discussion 475-477). - PubMed
-
- Boustead GB, Fowler S, Swamy R, et al. Stage, grade and pathological characteristics of bladder cancer in the UK: British Association of Urological Surgeons (BAUS) urological tumour registry. BJU Int. 2014;113:924–930. - PubMed
-
- Cambier S, Sylvester RJ, Collette L, et al. EORTC Nomograms and risk groups for predicting recurrence, progression, and disease-specific and overall survival in non-muscle-invasive stage Ta-T1 urothelial bladder cancer patients treated with 1-3 years of maintenance Bacillus Calmette-Guérin. Eur Urol. 2016;69:60–69. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
