

Portal Vein Embolization: History and Current Indications
- PMID: 29344514
- PMCID: PMC5757522
- DOI: 10.1159/000479474
Portal Vein Embolization: History and Current Indications
Abstract
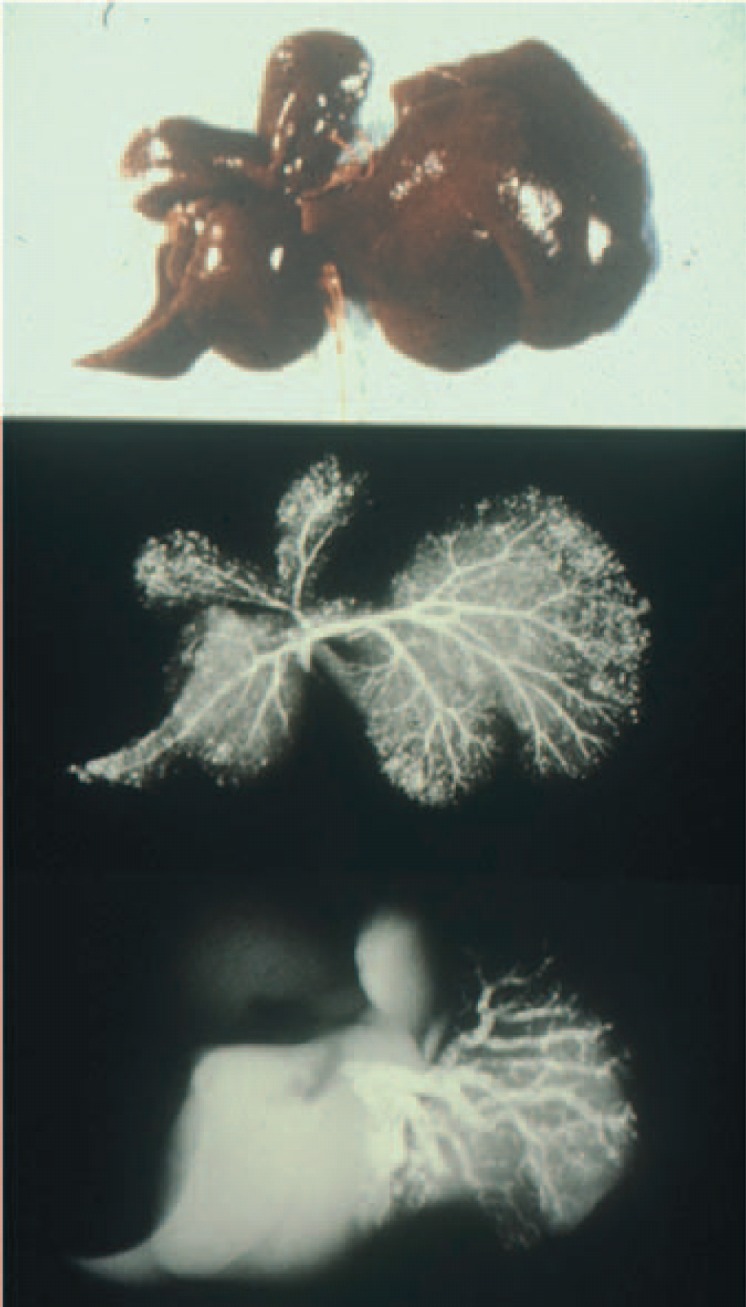
Portal vein embolization (PVE) was first adapted for patients undergoing major hepatectomy for hepatocellular carcinoma (HCC). In these patients, PVE caused hypertrophy of the unaffected liver and increased the volumetric ratio of future liver remnant (FLR) to total liver volume. 99mTechnetium-galactosyl human serum albumin (99mTc-GSA) scintigraphy revealed that PVE also induced a shift in hepatic function from the embolized part to the nonembolized part of the liver. Various hepatobiliary malignancies can be treated using PVE, and PVE is increasingly being used to expand the indication for major hepatectomy in patients with initially insufficient FLR volume or function. The indication for PVE is determined by the underlying liver function and standardized FLR volume. In patients with chronic hepatitis, the histologic inflammatory activity was negatively correlated with the increase in FLR volume, and PVE is not suitable for patients with high serum 7s collagen concentrations (>8 ng/ml). This finding may predict the efficacy of PVE. PVE before major hepatectomy can act as a tolerance test to avoid postoperative hepatic failure. PVE also improved long-term survival after liver resection in patients with HCC. Presently, PVE is a safe and useful treatment for patients undergoing major hepatectomy.
Keywords: Future liver remnant; Hepatectomy; Portal vein embolization.
Figures



References
-
- Honjo I, Suzuki T, Ozawa K, Takasan H, Kitamura O. Ligation of a branch of the portal vein for carcinoma of the liver. Am J Surg. 1975;130:296–302. - PubMed
-
- Kinoshita H, Sakai K, Hirohashi K, Igawa S, Yamasaki O, Kubo S. Preoperative portal vein embolization for hepatocellular carcinoma. World J Surg. 1986;10:803–808. - PubMed
-
- Makuuchi M, Thai BL, Takayasu K, Takayama T, Kosuge T, Gunven P, Yamazaki S, Hasegawa H, Ozaki H. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery. 1990;107:521–527. - PubMed
-
- Nagino M, Kamiya J, Kanai M, Uesaka K, Sano T, Yamamoto H, Hayakawa N, Nimura Y. Right trisegment portal vein embolization for biliary tract carcinoma: technique and clinical utility. Surgery. 2000;127:155–160. - PubMed
-
- Kubo S, Kinoshita H, Hirohashi K, Tanaka H, Tsukamoto T, Shuto T, Morimoto Y, Kanazawa A, Mikami S, Sakata C. Efficacy of preoperative portal vein embolization before major hepatectomy for patients with impaired liver function: a retrospective study. J Hepatobiliary Pancreat Surg. 1997;4:365–372.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
