

doi: 10.1210/js.2017-00389.
eCollection 2017 Dec 1.
A Practical Approach to Using Trend Arrows on the Dexcom G5 CGM System to Manage Children and Adolescents With Diabetes
Affiliations
- PMID: 29344578
- PMCID: PMC5760209
- DOI: 10.1210/js.2017-00389
Item in Clipboard
A Practical Approach to Using Trend Arrows on the Dexcom G5 CGM System to Manage Children and Adolescents With Diabetes
J Endocr Soc.
.
Abstract
After assessing previously published methods, we developed a practical approach to adjusting insulin doses using rtCGM trend arrows in pediatric patients with diabetes.
Keywords: continuous glucose monitoring; fine-tuning; insulin dose adjustment; insulin dosing; pediatric; type 1 diabetes.
Figures
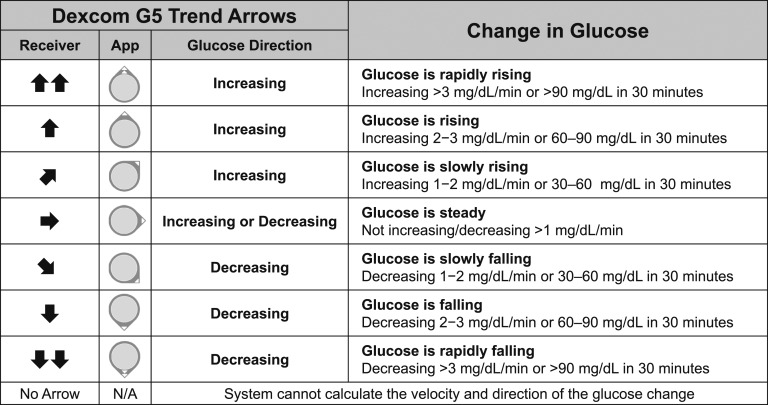
Dexcom G5 trend arrows. Dexcom G5 presents trend arrow data as icons on the Dexcom G5 Receiver and on the Dexcom G5 Mobile and Follow mobile apps (App) on compatible smart devices. According to the manufacturer, trend arrows indicate rates of glucose change (mg/dL per minute) and can be described as the anticipated glucose change in 30 minutes. Notably, the FLAT arrow (➡) indicates steady but does not indicate zero change. Note that trend arrows are determined by recent rtCGM measurements (generally the most recent 10 minutes of glucose values). In general, anticipated glucose may be less accurate when trying to predict changes over extended periods of time (e.g., beyond 20 to 30 minutes) due to the many factors that may influence glucose levels. Conversion: mg/dL × 0.0555 = mmol/L.

Other methods to adjust insulin doses using trend arrows. Three published methods for adjusting insulin dose using rtCGM trend arrow data are compared [DirecNet (Abbott system) [21], Scheiner (Medtronic and Dexcom systems) [22], and Pettus/Edelman (Dexcom system)] [23]. The DirecNet method takes total insulin dosage, including carbohydrate consumption (if any) into consideration. Scheiner and Pettus/Edelman methods are based on anticipated change in blood glucose with the Scheiner method being more conservative in insulin adjustment. Notably, the author of the Scheiner method has presented slightly modified values in recent presentations (personal communication) relative to past publication [22]. We use the more recently presented values in this comparison. All three require calculations beyond managing the correction and carbohydrate consumption. All three assume the patient has insulin requiring diabetes and is using rapid-acting insulin for meals and correction doses. Note that the recently published Klonoff/Kerr formula recommends adjusting insulin doses by 1, 1.5, or 2 U supplements/decrements for rates of change of 1 to 2, 2 to 3, and >3 mg/dL/min, respectively [24]. Conversion: mg/dL × 0.0555 = mmol/L.

New approach to adjust insulin doses using trend arrows in pediatric patients with diabetes. This figure outlines our approach to adjusting insulin doses using trend arrow data from the Dexcom G5 system in pediatric patients with diabetes receiving rapid acting insulin analogs. The approach is based on anticipated glucose change and typical insulin sensitivity ranges in pediatric patients that correspond to developmental stages. It should be noted that insulin sensitivity is generally greater in younger, prepubertal patients and decreases over time as youth age with decreasing insulin sensitivity associated with pubertal growth and development. The approach to adjusting insulin doses using trend arrows is suggested for premeal boluses and for corrections 3 or more hours following a meal. In general, the authors recommend avoiding adjustments using trend arrows immediately following meals due to the variability that ingested carbohydrates can have on trend arrows. Generally, one should begin with conservative adjustments to understand how the dose changes impact the individual. It is essential to understand that adjusting insulin doses using trend arrows does not replace but adds to standard calculations using ICR and CF. The approach assumes the patient has insulin requiring diabetes, is using rapid-acting insulin for meals and correction, and is using ICR and CF factors that have been accurately determined by the patient’s health care team (e.g., determining CF using the 1500 to 1800 rule) [36]. Conversion: mg/dL × 0.0555 = mmol/L. CF, correction factor in mg/dL, indicates glucose lowering per unit of rapid-acting insulin; U, units of rapid-acting insulin.

Sensitivity comparison of CF based methods to adjust insulin doses using trend arrows in pediatric patients. The figure is a visual comparison of insulin dose adjustments according to previous methods based on anticipated glucose (Scheiner and Pettus/Edelman) and our suggested approach based on insulin sensitivity ranges (Endocrine Society approach). The illustration shows that our approach aligns well with existing methods that indirectly use insulin sensitivity to adjust insulin doses while overcoming some of the limitations (e.g., a need for additional calculations and minimum increments possible for MDI-treated patients). Notably, our suggestion is relatively more conservative when applied to insulin-resistant individuals using lower CF ranges (e.g., <30) and more aggressive in the midrange (e.g., 40 to 75). However, one must consider that the calculations used in our approach are based on anticipated glucose at 30 minutes. When considering the anticipated glucose at 1 hour, the suggested insulin dose adjustments become more conservative. For example, a single UP trend arrow indicates that glucose is rising 2 to 3 mg/dL/min. At 30 minutes, the anticipated glucose would be 60 to 90 mg/dL higher. However, the anticipated glucose could be as much as 120 to 180 mg/dL at 60 minutes if unexposed to other perturbations. If a child’s CF was 60, our approach suggests adding 1 U of rapid-acting insulin to the premeal bolus. The additional 1 U of insulin would be expected to provide additional glucose lowering of 60 mg/dL over the 60 minutes. Given that the 60-minute anticipated glucose could potentially be much higher at 1 hour, our suggestion could be considered conservative. The expected glucose would be closer to target, postprandially, without overcorrecting and without increasing risk for hypoglycemia. As noted, these recommendations are starting points and should be readjusted as experience increases and responsiveness is observed and understood. Conversion: mg/dL × 0.0555 = mmol/L. CF, correction factor in mg/dL indicates glucose lowering per unit of rapid-acting insulin; U, units of rapid-acting insulin.
References
-
- Danne T, Bangstad HJ, Deeb L, Jarosz-Chobot P, Mungaie L, Saboo B, Urakami T, Battelino T, Hanas R; International Society for Pediatric and Adolescent Diabetes . ISPAD Clinical Practice Consensus Guidelines 2014. Insulin treatment in children and adolescents with diabetes. Pediatr Diabetes. 2014;15(Suppl 20):115–134. - PubMed
-
- Weinzimer SA, Tamborlane VW. Diabetes mellitus in children and adolescents In: Fonseca V, ed. Clinical Diabetes. Philadelphia, PA: Saunders Elsevier; 2006:505.
-
- Streisand R, Mackey ER, Elliot BM, Mednick L, Slaughter IM, Turek J, Austin A. Parental anxiety and depression associated with caring for a child newly diagnosed with type 1 diabetes: opportunities for education and counseling. Patient Educ Couns. 2008;73(2):333–338. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources