

Response to different furosemide doses predicts AKI progression in ICU patients with elevated plasma NGAL levels
- PMID: 29344743
- PMCID: PMC5772346
- DOI: 10.1186/s13613-018-0355-0
Response to different furosemide doses predicts AKI progression in ICU patients with elevated plasma NGAL levels
Abstract
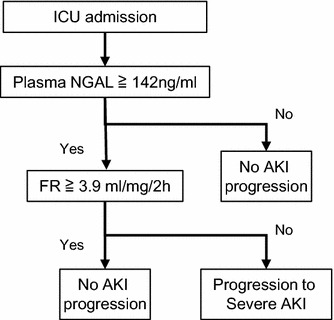
Background: Furosemide responsiveness (FR) is determined by urine output after furosemide administration and has recently been evaluated as a furosemide stress test (FST) for predicting severe acute kidney injury (AKI) progression. Although a standardized furosemide dose is required for FST, variable dosing is typically employed based on illness severity, including renal dysfunction in the clinical setting. This study aimed to evaluate whether FR with different furosemide doses can predict AKI progression. We further evaluated the combination of an AKI biomarker, plasma neutrophil gelatinase-associated lipocalin (NGAL), and FR for predicting AKI progression.
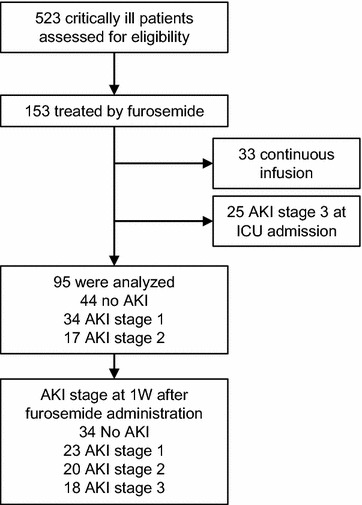
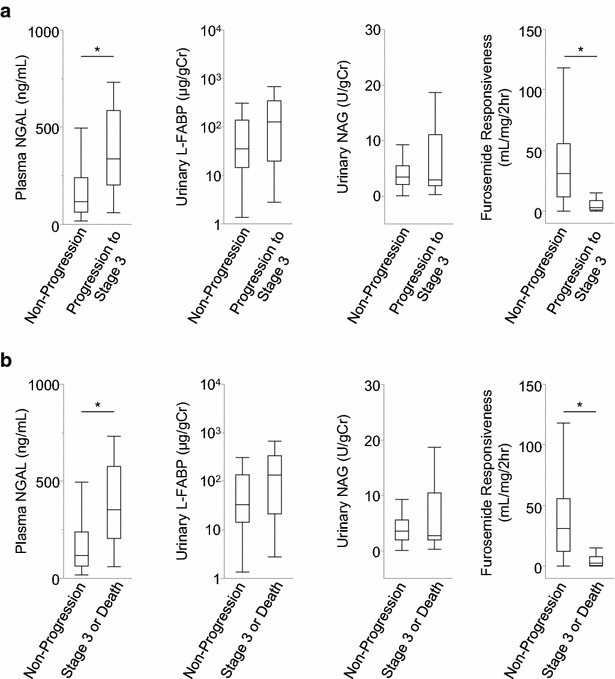
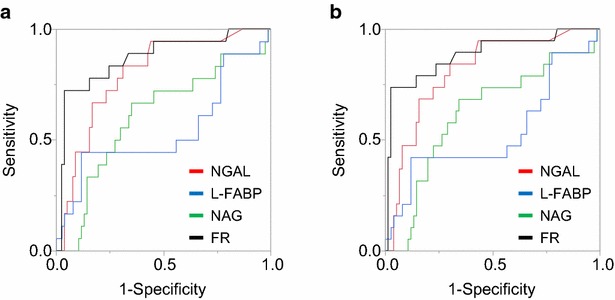
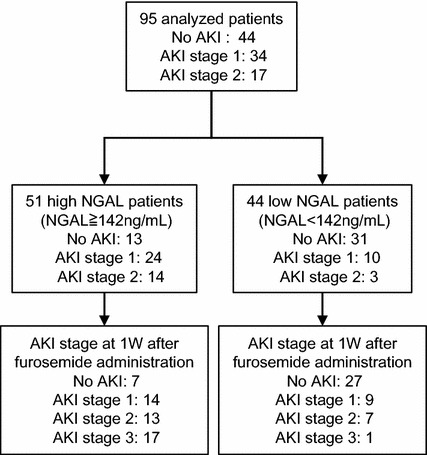
Results: We retrospectively analyzed 95 patients who were treated with bolus furosemide in our medical-surgical intensive care unit. Patients who had already developed AKI stage 3 were excluded. A total of 18 patients developed AKI stage 3 within 1 week. Receiver operating curve analysis revealed that the area under the curve (AUC) values of FR and plasma NGAL were 0.87 (0.73-0.94) and 0.80 (0.67-0.88) for AKI progression, respectively. When plasma NGAL level was < 142 ng/mL, only one patient developed stage 3 AKI, indicating that plasma NGAL measurements were sufficient to predict AKI progression. We further evaluated the performance of FR in 51 patients with plasma NGAL levels > 142 ng/mL. FR was associated with AUC of 0.84 (0.67-0.94) for AKI progression in this population with high NGAL levels.
Conclusions: Although different variable doses of furosemide were administered, FR revealed favorable efficacy for predicting AKI progression even in patients with high plasma NGAL levels. This suggests that a combination of FR and biomarkers can stratify the risk of AKI progression in a clinical setting.
Keywords: Acute kidney injury; Biomarkers; Diuretics; Intensive care unit; Progression.
Figures
References
-
- Iwagami M, Yasunaga H, Noiri E, Horiguchi H, Fushimi K, Matsubara T, et al. Current state of continuous renal replacement therapy for acute kidney injury in Japanese intensive care units in 2011: analysis of a national administrative database. Nephrol Dial Transplant. 2015;30:988–995. doi: 10.1093/ndt/gfv069. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
