

Laparoscopic conversion in colorectal cancer surgery; is there any improvement over time at a population level?
- PMID: 29344789
- PMCID: PMC5988765
- DOI: 10.1007/s00464-018-6042-2
Laparoscopic conversion in colorectal cancer surgery; is there any improvement over time at a population level?
Abstract
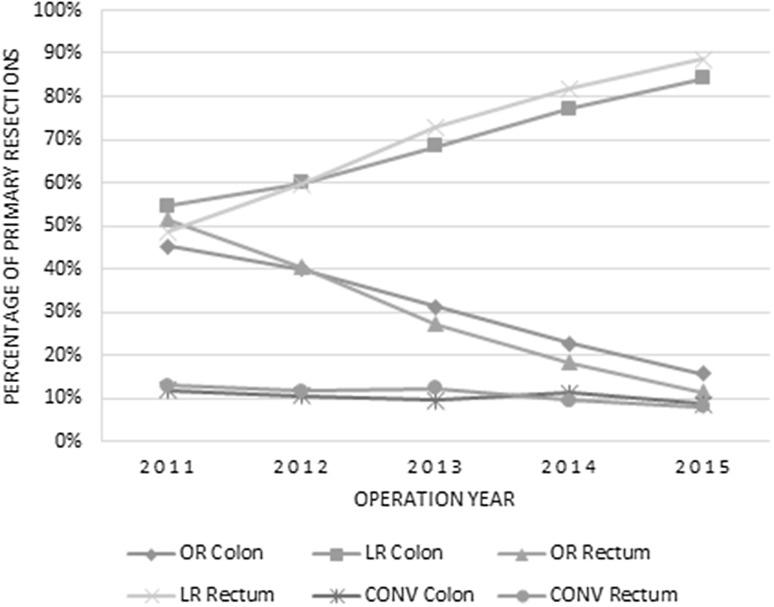
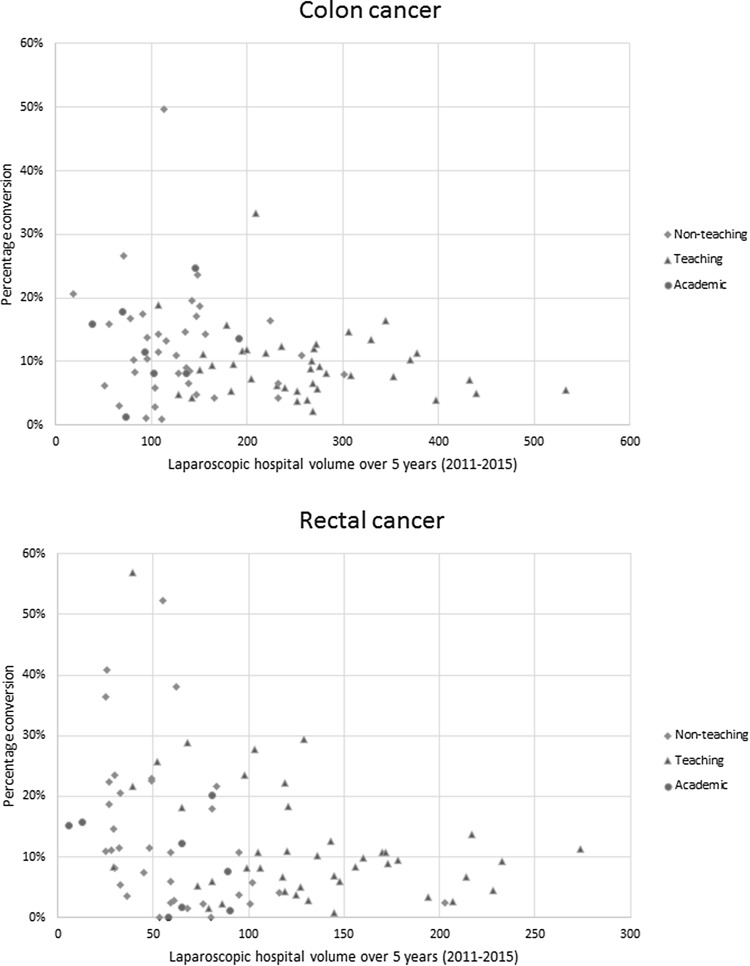
Conversion of laparoscopic colorectal cancer resection has been associated with worse outcome, but this might have been related to a learning curve effect. This study aimed to evaluate incidence, predictive factors and outcomes of laparoscopic conversion after the implementation phase of laparoscopic surgery at a population level. Patients undergoing elective resection of non-locally advanced, non-metastatic colorectal cancer between 2011 and 2015 were included. Data were extracted from the Dutch Surgical Colorectal Audit. Patients were grouped as laparoscopic completed (LR), laparoscopic converted (CONV) with further specification of timing (within or after 30 min) as registered in the DSCA, and open resection (OR). Uni- and multi-variate analyses were used to determine predictors of conversion and outcome (complicated course and mortality), with evaluation of trends over time. A total of 23,044 patients with colon cancer and 11,324 with rectal cancer were included. Between 2011 and 2015, use of laparoscopy increased from 55 to 84% in colon cancer, and from 49 to 89% in rectal cancer. Conversion rates decreased from 11.8 to 8.6% and from 13 to 8.0%, respectively. Laparoscopic hospital volume was independently associated with conversion rate. Only for colon cancer, the rate of complicated course was significantly higher after CONV compared to OR (adjusted odds ratio 1.486; 95% CI 1.298-1.702), and significantly higher after late (> 30 min) compared to early conversion (adjusted odds ratio 1.341; 1.046-1.719). There was no impact of CONV on mortality in both colon and rectal cancer. The use of laparoscopic colorectal cancer surgery increased to more than 80% at a national level, accompanied by a decrease in conversion which is significantly related to the laparoscopic hospital volume. Conversion was only associated with complicated course in colon cancer, especially when the reason for conversion consisted of an intra-operative complication, without affecting mortality.
Keywords: Colorectal cancer; Conversion; Improvements; Laparoscopic surgery; Learning.
Conflict of interest statement
Drs. Michael P. M. de Neree tot Babberich, Drs. Julia T. van Groningen, Prof Dr. Evelien Dekker, Prof. Dr. Theo Wiggers, Dr. Michel W. J. M. Wouters, Prof. Dr. Willem A. Bemelman, and Dr. Pieter J. Tanis have no conflict of interest or financial ties to disclose.
Figures
References
-
- Fleshman J, Branda M, Sargent DJ, Boller AM, George V, Abbas M, et al. Effect of laparoscopic-assisted resection vs open resection of stage II or III rectal cancer on pathologic outcomes: the ACOSOG Z6051 randomized clinical trial. JAMA. 2015;314:1346–1355. doi: 10.1001/jama.2015.10529. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
