

MSH6 and PMS2 germ-line pathogenic variants implicated in Lynch syndrome are associated with breast cancer
- PMID: 29345684
- PMCID: PMC6051923
- DOI: 10.1038/gim.2017.254
MSH6 and PMS2 germ-line pathogenic variants implicated in Lynch syndrome are associated with breast cancer
Abstract
Purpose: An association of Lynch syndrome (LS) with breast cancer has been long suspected; however, there have been insufficient data to address this question for each of the LS genes individually.
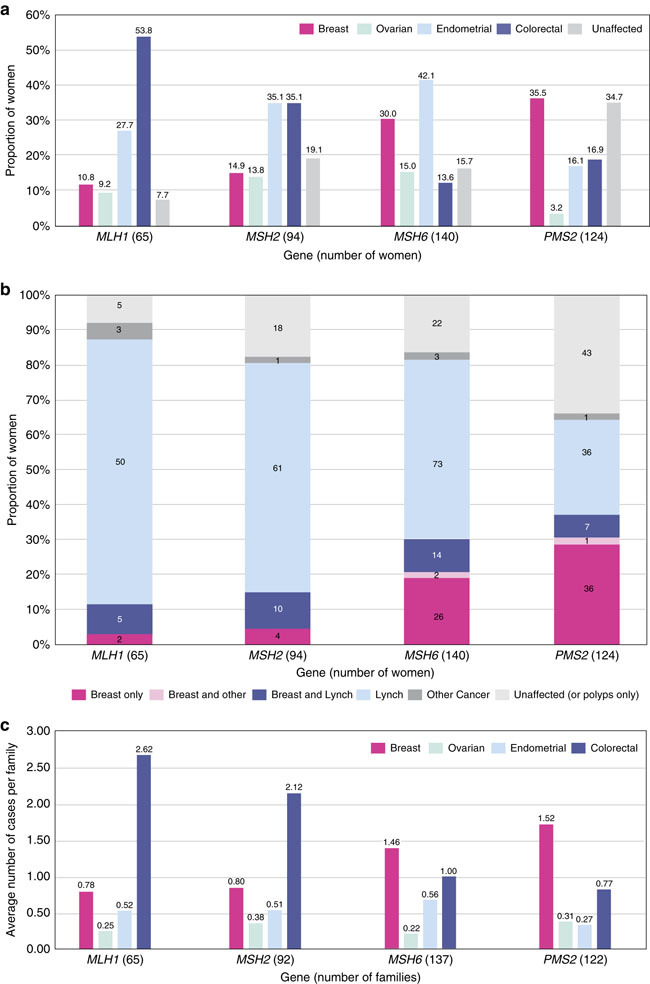
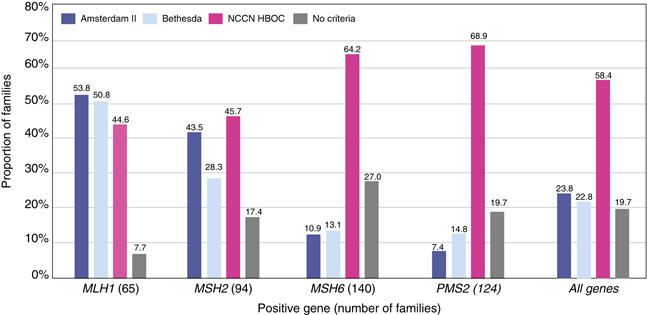
Methods: We conducted a retrospective review of personal and family history in 423 women with pathogenic or likely pathogenic germ-line variants in MLH1 (N = 65), MSH2 (N = 94), MSH6 (N = 140), or PMS2 (N = 124) identified via clinical multigene hereditary cancer testing. Standard incidence ratios (SIRs) of breast cancer were calculated by comparing breast cancer frequencies in our study population with those in the general population (Surveillance, Epidemiology, and End Results 18 data).
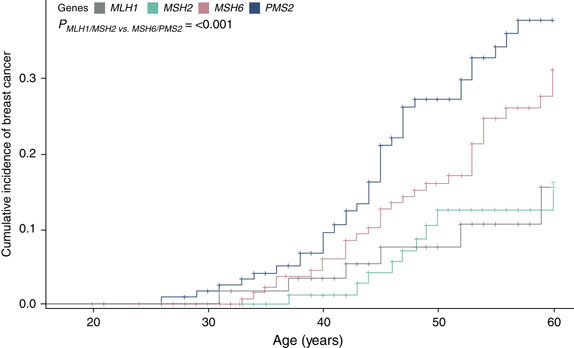
Results: When evaluating by gene, the age-standardized breast cancer risks for MSH6 (SIR = 2.11; 95% confidence interval (CI), 1.56-2.86) and PMS2 (SIR = 2.92; 95% CI, 2.17-3.92) were associated with a statistically significant risk for breast cancer whereas no association was observed for MLH1 (SIR = 0.87; 95% CI, 0.42-1.83) or MSH2 (SIR = 1.22; 95% CI, 0.72-2.06).
Conclusion: Our data demonstrate that two LS genes, MSH6 and PMS2, are associated with an increased risk for breast cancer and should be considered when ordering genetic testing for individuals who have a personal and/or family history of breast cancer.
Keywords: Lynch syndrome; MSH6; PMS2; breast cancer; mismatch repair.
Conflict of interest statement
M.E.R., S.A.J., L.R.S., M.L.M., A.R.S., B.M., and Z.X. are employed by GeneDx/BioReference Laboratories and have a salary as the only disclosure. W.K.C. is a former employee of BioReference Laboratories. K.S.H., R.T.K., and B.D.S. disclose stock and employment with GeneDx/BioReference Laboratories/Opko. The other authors declare no conflict of interest.
Figures
Comment in
-
Response to Roberts et al. 2018: is breast cancer truly caused by MSH6 and PMS2 variants or is it simply due to a high prevalence of these variants in the population?Genet Med. 2019 Jan;21(1):256-257. doi: 10.1038/s41436-018-0029-1. Epub 2018 May 24. Genet Med. 2019. PMID: 29795439 No abstract available.
-
Response to ten Broeke et al.Genet Med. 2019 Jan;21(1):258-259. doi: 10.1038/s41436-018-0031-7. Epub 2018 May 24. Genet Med. 2019. PMID: 29795440 Free PMC article. No abstract available.
-
Response to Evans et al.Genet Med. 2019 Aug;21(8):1880-1881. doi: 10.1038/s41436-018-0400-2. Epub 2018 Dec 19. Genet Med. 2019. PMID: 30563985 No abstract available.
-
Are women with pathogenic variants in PMS2 and MSH6 really at high lifetime risk of breast cancer?Genet Med. 2019 Aug;21(8):1878-1879. doi: 10.1038/s41436-018-0401-1. Epub 2018 Dec 14. Genet Med. 2019. PMID: 30631111 No abstract available.
-
Response to Roberts et al. 2018: cohort ascertainment and methods of analysis impact the association between cancer and genetic predisposition - the tale of breast cancer risk and Lynch syndrome genes MSH6/PMS2.Genet Med. 2019 Sep;21(9):2156-2157. doi: 10.1038/s41436-019-0471-8. Epub 2019 Feb 28. Genet Med. 2019. PMID: 30816297 No abstract available.
-
Response to Wang et al.Genet Med. 2019 Sep;21(9):2158. doi: 10.1038/s41436-019-0469-2. Epub 2019 Mar 1. Genet Med. 2019. PMID: 30824819 No abstract available.
References
-
- Risinger JI, Barrett JC, Watson P, Lynch HT, Boyd J. Molecular genetic evidence of the occurrence of breast cancer as an integral tumor in patients with the hereditary nonpolyposis colorectal carcinoma syndrome. Cancer. 1996;77:1836–1843. doi: 10.1002/(SICI)1097-0142(19960501)77:9<1836::AID-CNCR12>3.0.CO;2-0. - DOI - PubMed
-
- Anbazhagan R, Fujii H, Gabrielson E. Microsatellite instability is uncommon in breast cancer. Clin Cancer Res. 1999;5:839–844. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
