

Safety and pharmacokinetic profile of fixed-dose ivermectin with an innovative 18mg tablet in healthy adult volunteers
- PMID: 29346388
- PMCID: PMC5773004
- DOI: 10.1371/journal.pntd.0006020
Safety and pharmacokinetic profile of fixed-dose ivermectin with an innovative 18mg tablet in healthy adult volunteers
Abstract
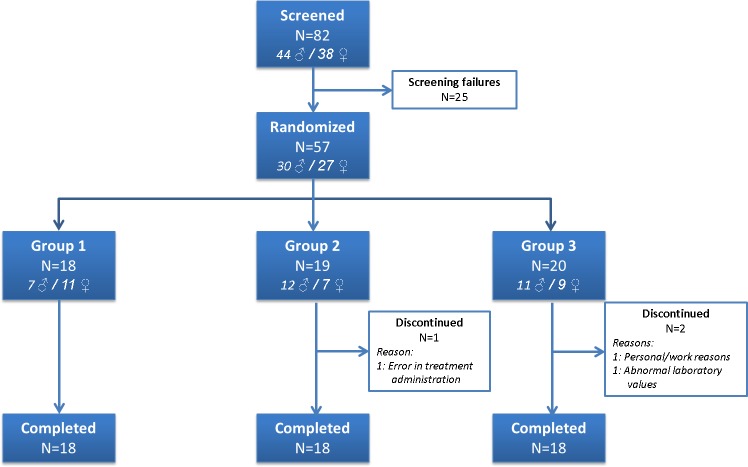
Ivermectin is a pivotal drug for the control of onchocerciasis and lymphatic filariasis, which is increasingly identified as a useful drug for the control of other Neglected Tropical Diseases. Its role in the treatment of soil transmitted helminthiasis through improved efficacy against Trichuris trichiura in combination with other anthelmintics might accelerate the progress towards breaking transmission. Ivermectin is a derivative of Avermectin B1, and consists of an 80:20 mixture of the equipotent homologous 22,23 dehydro B1a and B1b. Pharmacokinetic characteristics and safety profile of ivermectin allow to explore innovative uses to further expand its utilization through mass drug administration campaigns to improve coverage rates. We conducted a phase I clinical trial with 54 healthy adult volunteers who sequentially received 2 experimental treatments using a new 18 mg ivermectin tablet in a fixed-dose strategy of 18 and 36 mg single dose regimens, compared to the standard, weight based 150–200 μg/kg, regimen. Volunteers were recruited in 3 groups based on body weight. Plasma concentrations of ivermectin were measured through HPLC up to 168 hours post treatment. Safety data showed no significant differences between groups and no serious adverse events: headache was the most frequent adverse event in all treatment groups, none of them severe. Pharmacokinetic parameters showed a half-life between 81 and 91 h in the different treatment groups. When comparing the systemic bioavailability (AUC0t and Cmax) of the reference product (WA-ref) with the other two study groups using fixed doses, we observed an overall increase in AUC0t and Cmax for the two experimental treatments of 18 mg and 36 mg. Body mass index (BMI) and weight were associated with t1/2 and V/F, probably reflecting the high liposolubility of IVM with longer retention times proportional to the presence of more adipose tissue. Systemic exposure to ivermectin (AUC0t or Cmax) was not associated with BMI or weight in our study. These findings contribute to further understand the pharmacokinetic characteristics of ivermectin, highlighting its safety across different dosing regimens. They also correlate with known pharmacokinetic parameters showing stable levels of AUC and Cmax across a wide range of body weights, which justifies the strategy of fix dosing from a pharmacokinetic perspective.
Trial registration: ClinicalTrials.gov NCT03173742.
Conflict of interest statement
Yes. I have read the journal's policy and the authors of this manuscript have the following competing interests: EC and SG are members of Chemo Group, which includes Liconsa, the manufacturer of the study drug and Exeltis France, the funding source.
Figures



References
-
- Omura S, Crump A. Ivermectin: panacea for resource-poor communities? Trends Parasitol. 2014;30(9):445–55. doi: 10.1016/j.pt.2014.07.005 - DOI - PubMed
-
- Engels D. Neglected tropical diseases: A proxy for equitable development and shared prosperity. PLoS Negl Trop Dis. 2017;11(4):e0005419 doi: 10.1371/journal.pntd.0005419 - DOI - PMC - PubMed
-
- Chaccour C, Hammann F, Rabinovich NR. Ivermectin to reduce malaria transmission I. Pharmacokinetic and pharmacodynamic considerations regarding efficacy and safety. Malar J. 2017;16(1):161 doi: 10.1186/s12936-017-1801-4 - DOI - PMC - PubMed
-
- Gardon J, Gardon-Wendel N, Demanga N, Kamgno J, Chippaux JP, Boussinesq M. Serious reactions after mass treatment of onchocerciasis with ivermectin in an area endemic for Loa loa infection. Lancet. 1997;350(9070):18–22. doi: 10.1016/S0140-6736(96)11094-1 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
