

Management and outcomes of patients presenting with sepsis and septic shock to the emergency department during nursing handover: a retrospective cohort study
- PMID: 29347908
- PMCID: PMC5774108
- DOI: 10.1186/s12873-018-0155-8
Management and outcomes of patients presenting with sepsis and septic shock to the emergency department during nursing handover: a retrospective cohort study
Abstract
Background: Clinical handover is an important process for the transition of patient-care responsibility to the next healthcare provider, but it may divert the attention of the team away from active patients. This is challenging in the Emergency Department (ED) because of highly dynamic patient conditions and is likely relevant in conditions that requires time-sensitive therapies, such as sepsis. We aimed to examine the management and outcomes of patients presenting with sepsis and septic shock to the ED during nursing handover.
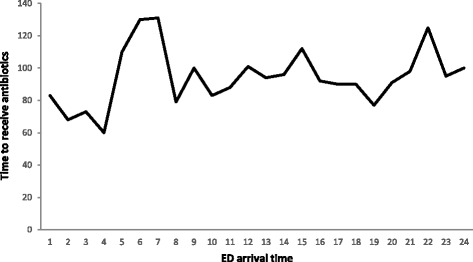
Methods: This retrospective cohort study was conducted at a 115-bed ED and more than 200,000 annual ED visits, within a 900-bed academic tertiary care center. Data on Surviving Sepsis Campaign (SSC) bundle elements and hospital mortality were collected for all ≥14-year-old patients who presented to the ED with a diagnosis of sepsis and septic shock between January 1, 2011 and October 30, 2013. Our primary outcome was time to antibiotics, were other SSC bundle elements and mortality counted as secondary outcomes. Patients were divided into two groups: 1) handover time group, comprising patients who presented an hour before or after the start of handover time (6-8 AM/PM), and 2) non-handover time group, comprising patients who presented over the remaining 20 h.
Results: During the study period, 1330 patients presented with sepsis or septic shock (228, handover time group; 1102, non-handover time group). No significant differences were found between the handover time and non-handover time groups, respectively, in median time to antibiotic administration (100 [interquartile range (IQR) 57-172] vs. 95 [IQR 50-190] minutes; P = 0.07), median time to serum lactate result (162 [IQR 108-246] vs. 156 [IQR 180-246] minutes; P = 0.33) and median time to obtain blood culture (54 [IQR 36-119] vs. 52 [IQR 28-103] minutes; P = 0.52), and hospital mortality rate (29.4% vs. 28.9%; P = 0.89).
Conclusion: No significant differences were found in median time of SSC bundle elements or hospital mortality between patients who presented during the handover and non-handover times.
Keywords: Handover; Nursing; Sepsis.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of Ministry of National Guard-Health affairs, and given this study does not disclose patient identity and pose no risk to the patients the informed consent requirement was waived.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
