

Cost-effectiveness of prostate cancer screening: a systematic review of decision-analytical models
- PMID: 29347916
- PMCID: PMC5773135
- DOI: 10.1186/s12885-017-3974-1
Cost-effectiveness of prostate cancer screening: a systematic review of decision-analytical models
Abstract
Background: There is ongoing debate about the harms and benefits of a national prostate cancer screening programme. Several model-based cost-effectiveness analyses have been developed to determine whether the benefits of prostate cancer screening outweigh the costs and harms caused by over-detection and over-treatment, and the different approaches may impact results.
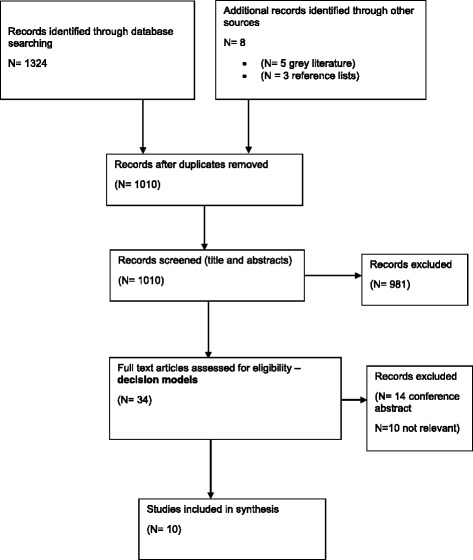
Methods: To identify models of prostate cancer used to assess the cost-effectiveness of prostate cancer screening strategies, a systematic review of articles published since 2006 was conducted using the NHS Economic Evaluation Database, Medline, EMBASE and HTA databases. The NICE website, UK National Screening website, reference lists from relevant studies were also searched and experts contacted. Key model features, inputs, and cost-effectiveness recommendations were extracted.
Results: Ten studies were included. Four of the studies identified some screening strategies to be potentially cost-effective at a PSA threshold of 3.0 ng/ml, including single screen at 55 years, annual or two yearly screens starting at 55 years old, and delayed radical treatment. Prostate cancer screening was modelled using both individual and cohort level models. Model pathways to reflect cancer progression varied widely, Gleason grade was not always considered and clinical verification was rarely outlined. Where quality of life was considered, the methods used did not follow recommended practice and key issues of overdiagnosis and overtreatment were not addressed by all studies.
Conclusion: The cost-effectiveness of prostate cancer screening is unclear. There was no consensus on the optimal model type or approach to model prostate cancer progression. Due to limited data availability, individual patient-level modelling is unlikely to increase the accuracy of cost-effectiveness results compared with cohort-level modelling, but is more suitable when assessing adaptive screening strategies. Modelling prostate cancer is challenging and the justification for the data used and the approach to modelling natural disease progression was lacking. Country-specific data are required and recommended methods used to incorporate quality of life. Influence of data inputs on cost-effectiveness results need to be comprehensively assessed and the model structure and assumptions verified by clinical experts.
Keywords: Cost-effectiveness; PSA test; Prostate cancer; Screening; Systematic review.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Prostate Cancer Incidence Statistics [http://www.cancerresearchuk.org/health-professional/cancer-statistics/st...]. Accessed 1 Mar 2017.
-
- Rosario DJ, Lane JA, Metcalfe C, Donovan JL, Doble A, Goodwin L, Davis M, Catto JW, Avery K, Neal DE, et al. Short term outcomes of prostate biopsy in men tested for cancer by prostate specific antigen: prospective evaluation within ProtecT study. BMJ. 2012;344:d7894. doi: 10.1136/bmj.d7894. - DOI - PMC - PubMed
-
- Ahmed HU, El-Shater Bosaily A, Brown LC, Gabe R, Kaplan R, Parmar MK, Collaco-Moraes Y, Ward K, Hindley RG, Freeman A, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet. 2017;389(10071):815–822. doi: 10.1016/S0140-6736(16)32401-1. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- 15064/CRUK_/Cancer Research UK/United Kingdom
- 24432/CRUK_/Cancer Research UK/United Kingdom
- C11043/A4286, C18281/A8145, C18281/A11326, C18281/A15064, C18281/A24432/CRUK_/Cancer Research UK/United Kingdom
- C11043/A4286, C18281/A8145, C18281/A11326, and C18281/A15064, C18281/A24432/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
