

A five-year retrospective study of the epidemiological characteristics and visual outcomes of pediatric ocular trauma
- PMID: 29347941
- PMCID: PMC5774107
- DOI: 10.1186/s12886-018-0676-7
A five-year retrospective study of the epidemiological characteristics and visual outcomes of pediatric ocular trauma
Abstract
Background: Pediatric trauma can lead to serious visual impairment as a result of the trauma itself or secondary to amblyopia. Precise data on epidemiological characteristics and visual outcomes of pediatric ocular injuries are valuable for the prevention of monocular blindness.
Methods: A total of 268 cases of pediatric ocular trauma admitted to the Department of Ophthalmology of the Lithuanian University of Health Sciences Hospital from January 2008 to December 2013 were retrospectively reviewed. Data analysed included age, sex, cause, type and treatment of injury, initial and final visual acuity (VA) and tissues involvement. Eye injuries were classified by Birmingham Eye Trauma Terminology (BETT) and Ocular Trauma Classification System (OTCS).
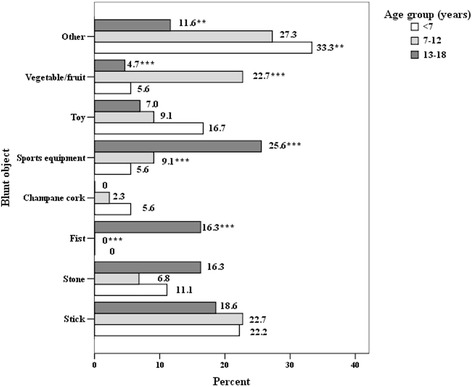
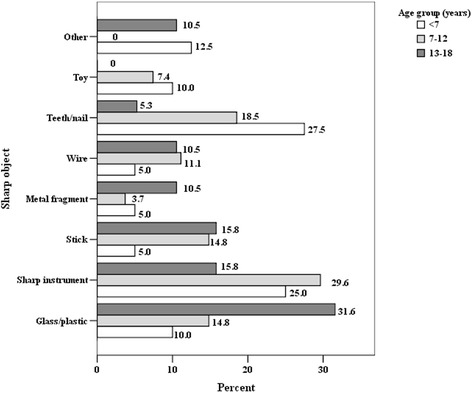
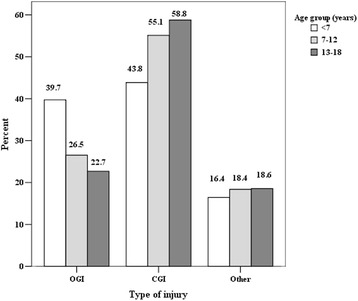
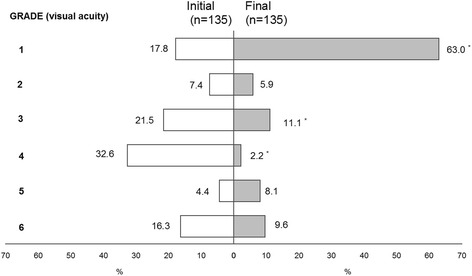
Results: The age of children ranged from 6 months to 17.5 years. Boys were more likely to suffer ocular injury than girls. Home was the leading place of eye injury (60.4%), followed by outdoors (31.7%), school (5.2%) and sporting area (2.2%). The highest percentage of eye injuries in children were caused by blunt (40.3%) and sharp objects (29.9%), followed by burns (9.3%), falls (6.7%), explosions (4.5%), fireworks (4.1%), gunshots (1.9%) and traffic accidents (0.7%). Closed globe injury (CGI) was the most common type of eye injury (53.4%). CGI were noted to be higher in children aged 13-18 years, while open globe injury (OGI) were higher in the pre-school age group. Injury of grade 4 and grade 5 were more common in OGI, while grade 1 and grade 2 predominated in cases of CGI. Hypotony, traumatic cataract, iris laceration, vitreous prolapse and uveitis were the most common presentations of OGI, while hyphema, secondary glaucoma and retinal edema were significantly related with CGI. Final diagnoses contributing to poor final visual outcome such as corneal scar corneal opacity, hypotony, aphakia, and retinal detachment were statistically significant related only with OGI. Overall, 65.63% of children regained good visual acuity (VA ≥ 0.5), but for 18.4% of them, the trauma resulted in severe visual impairment (VA ≤ 0.1).
Conclusion: Ocular trauma in children still remains an important preventable cause of ocular morbidity. This study provides data indicating that ophthalmological injuries are a significant cause of visual impairment in children.
Keywords: Ocular injury; Pediatric eye trauma; Visual outcome.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective study adhered to the tenets of the Declaration of Helsinki and received the approval from the Regional Committee of Bioethics (N° BEC-MF-679).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Kaur A, Agrawal A. Paediatric ocular trauma. Curr Sci. 2005;89:43–46.
-
- Brophy M, Sinclair SA, Hostetler SG, Xiang H. Pediatric eye – related hospitalizations in the United States. Pediatrics. 2006;117 10.1542/peds.2005-1950. - PubMed
-
- Lee CH, Su WY, Lee L, Yang ML. Pediatric ocular trauma in Taiwan. Chang Gung Med J. 2008;31(1):59–65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
