

Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study
- PMID: 29347982
- PMCID: PMC5774130
- DOI: 10.1186/s13054-017-1926-4
Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study
Abstract
Background: Providing supplemental oxygen is fundamental in the management of mechanically ventilated patients. Increasing amounts of data show worse clinical outcomes associated with hyperoxia. However, these previous data in the critically ill have not focused on outcomes associated with brief hyperoxia exposure immediately after endotracheal intubation. Therefore, the objectives of this study were to evaluate the impact of isolated early hyperoxia exposure in the emergency department (ED) on clinical outcomes among mechanically ventilated patients with subsequent normoxia in the intensive care unit (ICU).
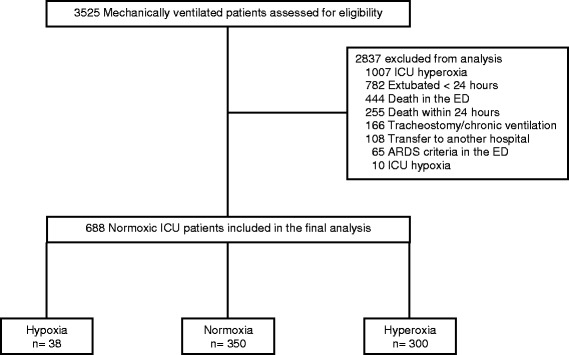
Methods: This was an observational cohort study conducted in the ED and ICUs of an academic center in the USA. Mechanically ventilated normoxic (partial pressure of arterial oxygen (PaO2) 60-120 mm Hg) ICU patients with mechanical ventilation initiated in the ED were studied. The cohort was categorized into three oxygen exposure groups based on PaO2 values obtained after ED intubation: hypoxia, normoxia, and hyperoxia (defined as PaO2 < 60 mmHg, PaO2 60-120 mm Hg, and PaO2 > 120 mm Hg, respectively, based on previous literature).
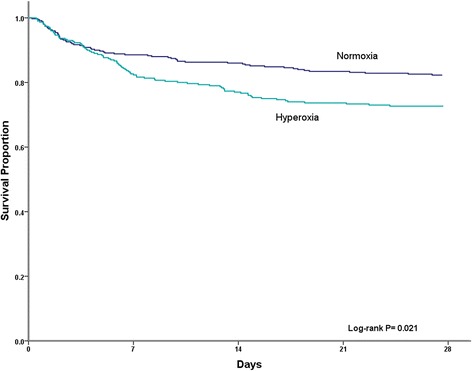
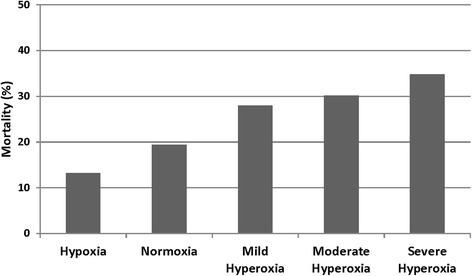
Results: A total of 688 patients were included. ED normoxia occurred in 350 (50.9%) patients, and 300 (43.6%) had exposure to ED hyperoxia. The ED hyperoxia group had a median (IQR) ED PaO2 of 189 mm Hg (146-249), compared to an ED PaO2 of 88 mm Hg (76-101) in the normoxia group, P < 0.001. Patients with ED hyperoxia had greater hospital mortality (29.7%), when compared to those with normoxia (19.4%) and hypoxia (13.2%). After multivariable logistic regression analysis, ED hyperoxia was an independent predictor of hospital mortality (adjusted OR 1.95 (1.34-2.85)).
Conclusions: ED exposure to hyperoxia is common and associated with increased mortality in mechanically ventilated patients achieving normoxia after admission. This suggests that hyperoxia in the immediate post-intubation period could be particularly injurious, and targeting normoxia from initiation of mechanical ventilation may improve outcome.
Keywords: Emergency department; Hyperoxia; Mechanical ventilation.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Human Research Protection Office of Washington University in St. Louis under waiver of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Periintubation Ventilation and Oxygenation of Acutely Ill Patients.Am J Respir Crit Care Med. 2020 Apr 1;201(7):856-858. doi: 10.1164/rccm.201904-0904RR. Am J Respir Crit Care Med. 2020. PMID: 32027808 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
