

Impaired Recovery of Left Ventricular Function in Patients With Cardiomyopathy and Left Bundle Branch Block
- PMID: 29348023
- PMCID: PMC8352572
- DOI: 10.1016/j.jacc.2017.11.020
Impaired Recovery of Left Ventricular Function in Patients With Cardiomyopathy and Left Bundle Branch Block
Erratum in
-
Correction.J Am Coll Cardiol. 2018 Mar 20;71(11):1296. doi: 10.1016/j.jacc.2018.02.027. J Am Coll Cardiol. 2018. PMID: 29544619 No abstract available.
Abstract
Background: Patients with left bundle branch block (LBBB) often respond to cardiac resynchronization therapy (CRT) with left ventricular ejection fraction (LVEF) improvement. Guideline-directed medical therapy (GDMT), not CRT, is first-line therapy for patients with reduced LVEF with LBBB. However, there are little data on how patients with reduced LVEF and LBBB respond to GDMT.
Objectives: This study examined patients with cardiomyopathy and sought to assess rates of LVEF improvement for patients with LBBB compared to other QRS morphologies.
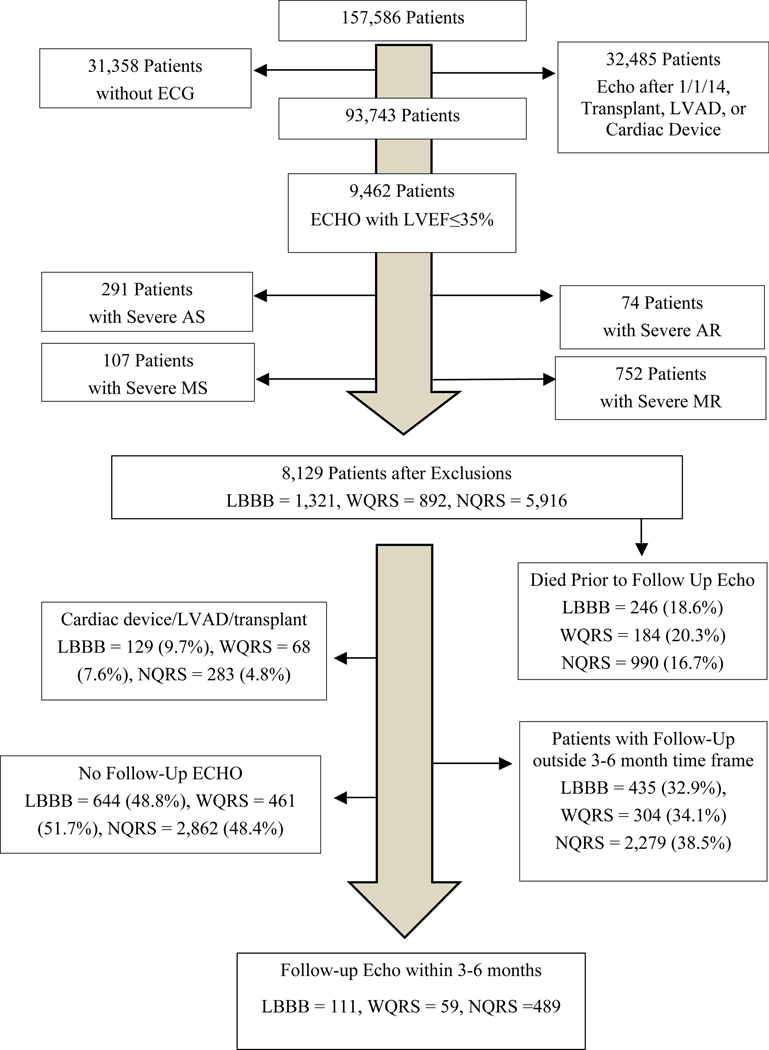
Methods: Using data from the Duke Echocardiography Laboratory Database, the study identified patients with baseline electrocardiography and LVEF ≤35% who had a follow-up LVEF 3 to 6 months later. The study excluded patients with severe valve disease, a cardiac device, left ventricular assist device, or heart transplant. QRS morphology was classified as LBBB, QRS duration <120 ms (narrow QRS duration), or a wide QRS duration ≥120 ms but not LBBB. Analysis of variance testing compared mean change in LVEF among the 3 groups with adjustment for significant comorbidities and GDMT.
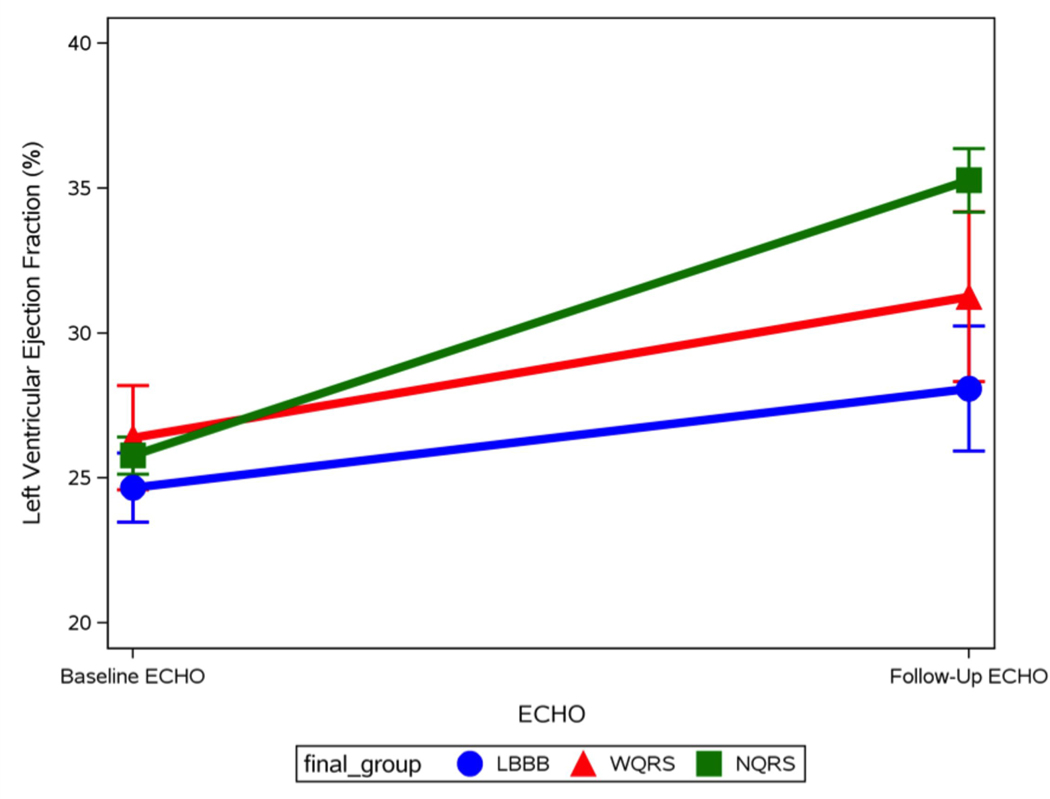
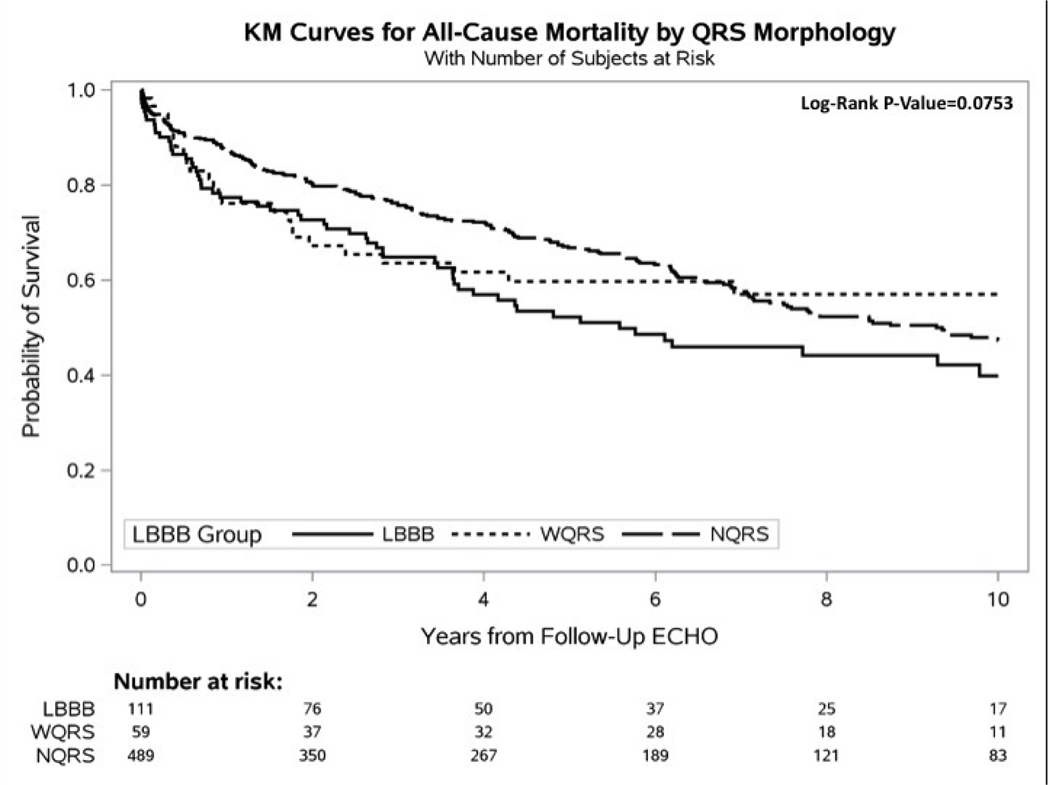
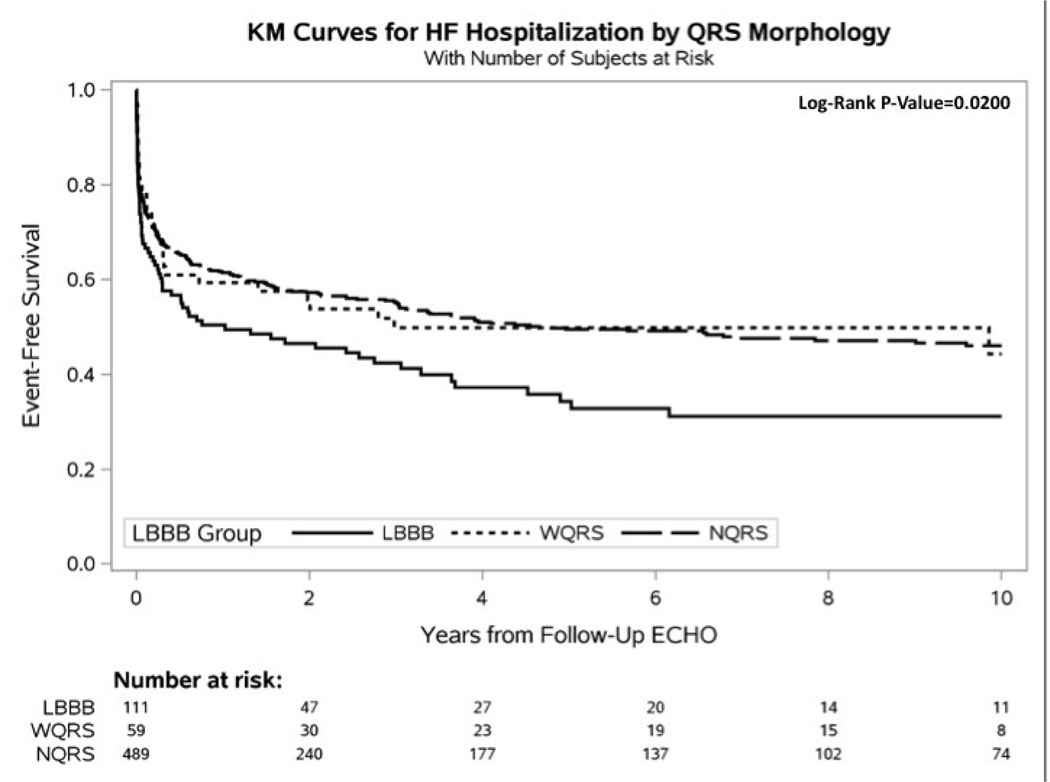
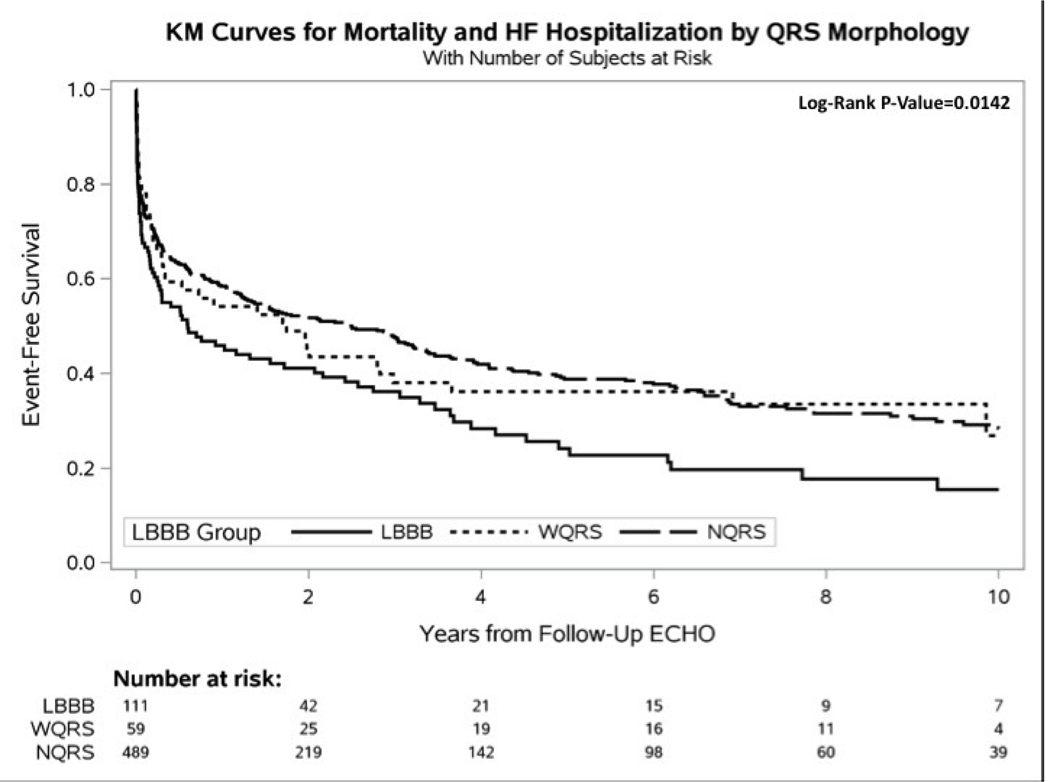
Results: There were 659 patients that met the criteria: 111 LBBB (17%), 59 wide QRS duration ≥120 ms but not LBBB (9%), and 489 narrow QRS duration (74%). Adjusted mean increase in LVEF over 3 to 6 months in the 3 groups was 2.03%, 5.28%, and 8.00%, respectively (p < 0.0001). Results were similar when adjusted for interim revascularization and myocardial infarction. Comparison of mean LVEF improvement between patients with LBBB on GDMT and those not on GDMT showed virtually no difference (3.50% vs. 3.44%). The combined endpoint of heart failure hospitalization or mortality was highest for patients with LBBB.
Conclusions: LBBB is associated with a smaller degree of LVEF improvement compared with other QRS morphologies, even with GDMT. Some patients with LBBB may benefit from CRT earlier than guidelines currently recommend.
Keywords: guideline directed medical therapy; heart failure; left bundle branch block; left ventricular functional recovery.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cardiomyopathy and Left Bundle Branch Block: A Farewell to Drugs?J Am Coll Cardiol. 2018 Jan 23;71(3):318-320. doi: 10.1016/j.jacc.2017.11.039. J Am Coll Cardiol. 2018. PMID: 29348024 No abstract available.
-
Left Bundle Branch Block-Associated Cardiomyopathies and Early Cardiac Resynchronization Therapy: Conceptualizing a Tailored Approach.J Am Coll Cardiol. 2018 May 1;71(17):1943-1944. doi: 10.1016/j.jacc.2018.02.060. J Am Coll Cardiol. 2018. PMID: 29699624 No abstract available.
-
Dyssynchrony-Induced Cardiomyopathy.J Am Coll Cardiol. 2018 May 1;71(17):1944-1945. doi: 10.1016/j.jacc.2018.02.063. J Am Coll Cardiol. 2018. PMID: 29699625 No abstract available.
-
Reply: Early Cardiac Resynchronization Therapy for Left Bundle Branch Block-Associated Cardiomyopathies.J Am Coll Cardiol. 2018 May 1;71(17):1945-1946. doi: 10.1016/j.jacc.2018.03.011. J Am Coll Cardiol. 2018. PMID: 29699626 No abstract available.
Similar articles
-
Left bundle branch block-induced left ventricular remodeling and its potential for reverse remodeling.J Interv Card Electrophysiol. 2018 Aug;52(3):343-352. doi: 10.1007/s10840-018-0407-2. Epub 2018 Jul 17. J Interv Card Electrophysiol. 2018. PMID: 30019271 Review.
-
New-onset left bundle branch block-associated idiopathic nonischemic cardiomyopathy and left ventricular ejection fraction response to guideline-directed therapies: The NEOLITH study.Heart Rhythm. 2016 Apr;13(4):933-42. doi: 10.1016/j.hrthm.2015.12.020. Epub 2015 Dec 11. Heart Rhythm. 2016. PMID: 26688064
-
Response to cardiac resynchronization therapy in non-ischemic cardiomyopathy is unrelated to medical therapy.Clin Cardiol. 2019 Jan;42(1):143-150. doi: 10.1002/clc.23123. Epub 2018 Dec 15. Clin Cardiol. 2019. PMID: 30467886 Free PMC article.
-
Machine Learning of 12-Lead QRS Waveforms to Identify Cardiac Resynchronization Therapy Patients With Differential Outcomes.Circ Arrhythm Electrophysiol. 2020 Jul;13(7):e008210. doi: 10.1161/CIRCEP.119.008210. Epub 2020 Jun 14. Circ Arrhythm Electrophysiol. 2020. PMID: 32538136 Free PMC article.
-
LBBB and heart failure-Relationships among QRS amplitude, duration, height, LV mass, and sex.J Cardiovasc Electrophysiol. 2024 Mar;35(3):583-591. doi: 10.1111/jce.16097. Epub 2023 Oct 9. J Cardiovasc Electrophysiol. 2024. PMID: 37811553 Review.
Cited by
-
Rationale and Study Design of the Withdrawal of Spironolactone for Heart Failure with Improved Left Ventricular Ejection Fraction.Int J Heart Fail. 2021 Jan 14;3(1):51-58. doi: 10.36628/ijhf.2020.0044. eCollection 2021 Jan. Int J Heart Fail. 2021. PMID: 36263115 Free PMC article.
-
Predicting the Development of Reduced Left Ventricular Ejection Fraction in Patients With Left Bundle Branch Block.Am J Cardiol. 2020 Dec 15;137:39-44. doi: 10.1016/j.amjcard.2020.09.034. Epub 2020 Sep 28. Am J Cardiol. 2020. PMID: 32998010 Free PMC article.
-
Left bundle branch block-induced left ventricular remodeling and its potential for reverse remodeling.J Interv Card Electrophysiol. 2018 Aug;52(3):343-352. doi: 10.1007/s10840-018-0407-2. Epub 2018 Jul 17. J Interv Card Electrophysiol. 2018. PMID: 30019271 Review.
-
Myocardial recovery after cardiac resynchronization therapy in left bundle branch block-associated idiopathic nonischemic cardiomyopathy: A NEOLITH II substudy.Ann Noninvasive Electrocardiol. 2019 Mar;24(2):e12603. doi: 10.1111/anec.12603. Epub 2018 Sep 28. Ann Noninvasive Electrocardiol. 2019. PMID: 30267454 Free PMC article.
-
Prevalence, clinical and instrumental features of left bundle branch block-induced cardiomyopathy: the CLIMB registry.ESC Heart Fail. 2021 Dec;8(6):5589-5593. doi: 10.1002/ehf2.13568. Epub 2021 Sep 12. ESC Heart Fail. 2021. PMID: 34510787 Free PMC article.
References
-
- Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 2013;62:e147–239. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg 2014;148:e1–e132. - PubMed
-
- Patel MR, Dehmer GJ, Hirshfeld JW et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2009;53:530–53. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. The New England journal of medicine 2009;361:1329–38. - PubMed
-
- Tang AS, Wells GA, Talajic M et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med 2010;363:2385–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
