

An immunohistochemical analysis of folate receptor beta expression and distribution in giant cell arteritis - a pilot study
- PMID: 29348986
- PMCID: PMC5768896
An immunohistochemical analysis of folate receptor beta expression and distribution in giant cell arteritis - a pilot study
Abstract
Background: Giant cell arteritis (GCA) is a chronic vasculitis of large and medium vessels in which no targetable biomarkers exist to allow selective treatment, predict disease activity and monitor therapeutic responses. The accessibility of the temporal artery (TA) for biopsy allows morphologic studies to characterize macrophages and T cells in the microenvironment of the arterial wall. We evaluated the expression of folate receptor beta (FRB), a candidate diagnostic/therapeutic biomarker, compared its expression with key macrophage markers and correlated it with GCA severity.
Methods: Formalin-fixed paraffin-embedded tissue sections were examined from 6 patients with GCA and 2 controls. Immunohistochemistry was performed using FRB, ETB, CD68 and CD3 antibodies to evaluate for activated macrophages and T cells, assess FRB distribution along the intima, media and adventitial layers and composition of inflammatory infiltrates. We compared the expression of FRB, ETB and CD68 in GCA versus negative controls and in severe (with visual loss) versus mild (without visual loss) disease.
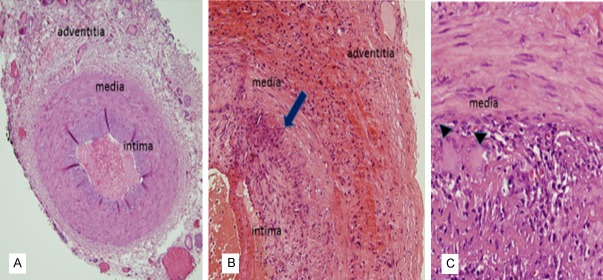
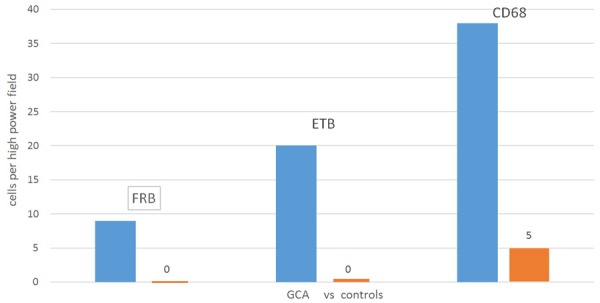
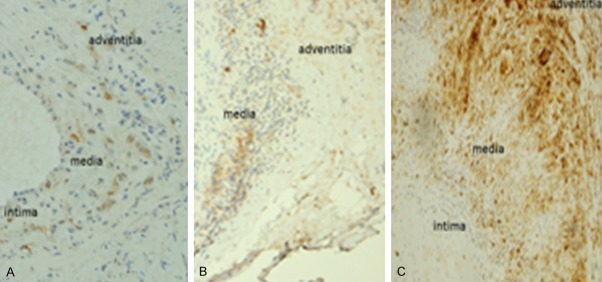
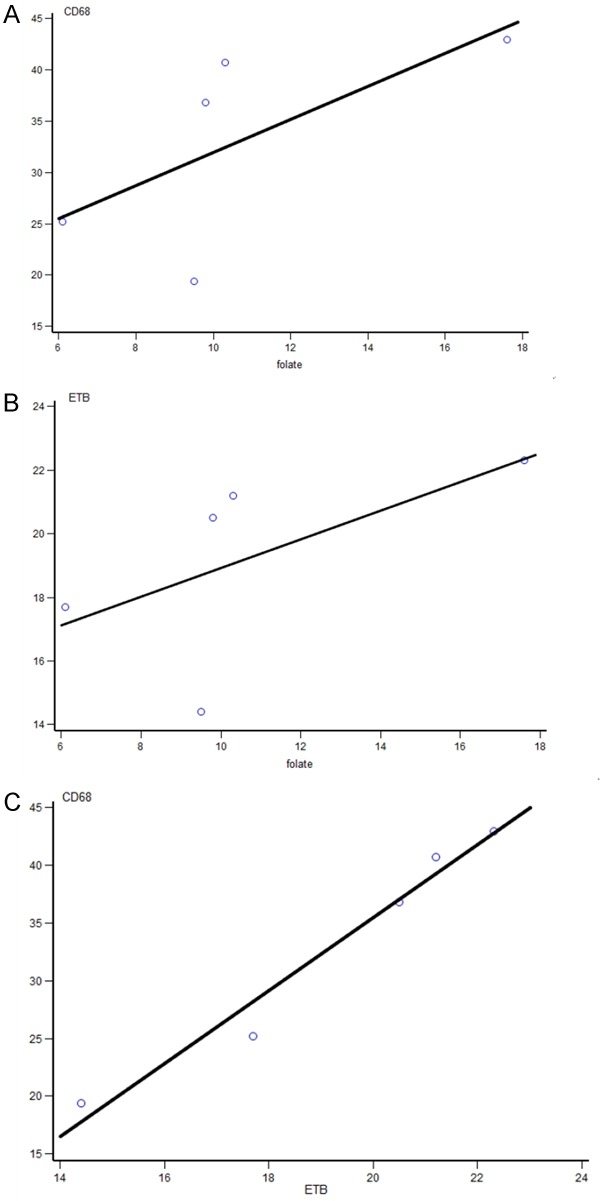
Results: In GCA, moderate to severe inflammation was accompanied by >90% destruction of the internal elastic lamina. Macrophages comprised 36.3 ± 4.1% while CD3+ lymphocytes accounted for 61.7 ± 4.1% of total leukocytes. FRB was selectively expressed in macrophages and localized to the adventitia. GCA patients had marginally increased median FRB (9.8 cells/hpf vs. 0; p=0.095), ETB (20.5 vs. 0; p=0.095) and CD68 (38.8 vs. 5; p=0.071) expression versus controls. ETB was found in endothelial cells, smooth muscle cells and macrophages in intima/media. FRB positively correlated with ETB (r=0.90; p-0.037) and CD68 levels (r=0.90; p=0.037). ETB expression positively correlated with CD68 (r=1.0; p<0.0001). There was no difference in FRB between severe and mild GCA.
Conclusion: FRB is a potential diagnostic and therapeutic biomarker with restricted expression in GCA macrophages. FRB+ macrophages localized to the adventitia and their expression correlated with ETB and CD68 macrophages, suggesting that they contribute to GCA pathogenesis.
Keywords: Giant cell arteritis; folate receptor beta; macrophages.
Conflict of interest statement
None.
Figures
References
-
- Evans JM, Hunder GG. Polymyalgia rheumatica and giant cell arteritis. Rheum Dis Clin North Am. 2000;26:493–515. - PubMed
-
- Hunder GG. Giant cell arteritis and polymyalgia rheumatica. Med Clin North Am. 1997;81:195–219. - PubMed
-
- Lobato-Berezo A, Alcalde-Villar M, Imbernon-Moya A, Martinez-Perez M, Aguilar-Martinez A, Collado-Ramos P. Tongue necrosis: an unusual clinical presentation of giant cell arteritis. Arthritis Rheumatol. 2014;66:2803. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials