

Meniscal Repair With Fibrin Clot Augmentation
- PMID: 29348998
- PMCID: PMC5766256
- DOI: 10.1016/j.eats.2017.08.006
Meniscal Repair With Fibrin Clot Augmentation
Abstract
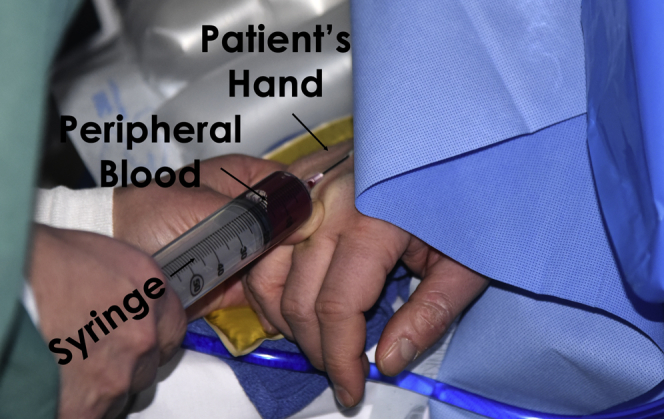
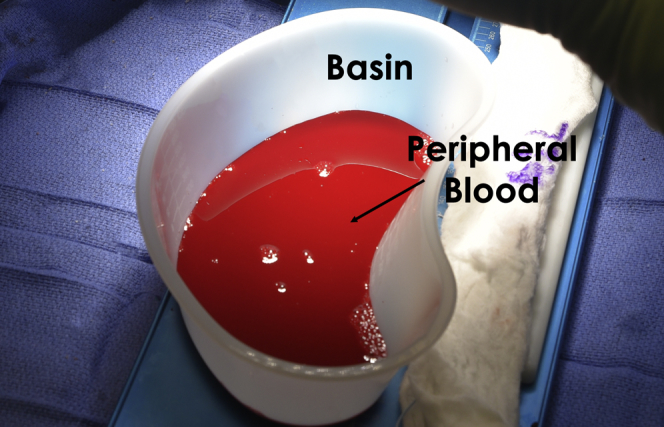
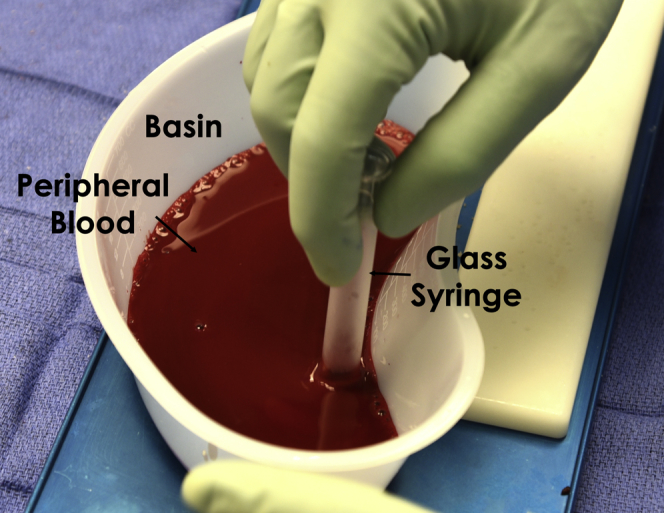
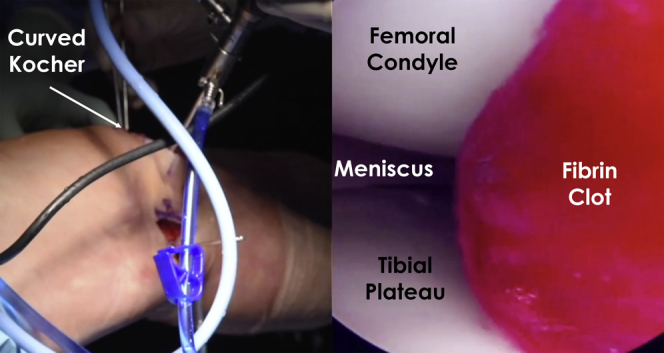
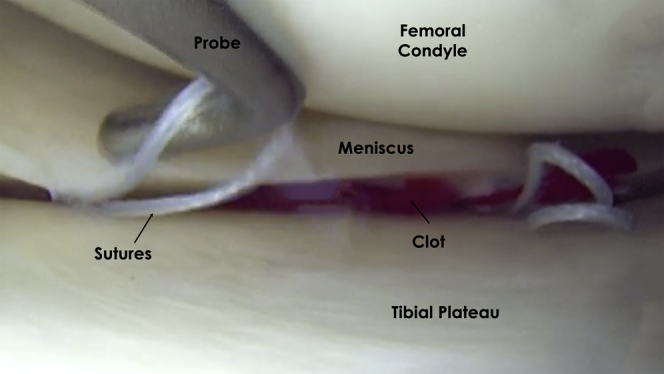
Meniscal injuries and meniscal loss are associated with changes in knee kinematics and loading, ultimately leading to poor functional outcomes and increased risk of progression to osteoarthritis. Biomechanical studies have shown restored knee function, and clinical studies have reported improved outcomes and decreased risk of osteoarthritis after meniscal repair. This has led orthopaedic surgeons to try and save the meniscus by repair whenever possible, as shown by increasing incidence of meniscal repair surgeries. Historically, meniscal lesions, particularly those greater in size and located in the white-white region of the meniscus, have been shown to have poor healing. In recent years, there has been an increasing interest in the use of biologic agents to help stimulate and expedite healing in traditionally more avascular tissue. Preliminary results for biologic therapeutic agents, such as platelet rich plasma and bone marrow aspirate concentrate, have been encouraging. However, these options are more demanding in regard to time, financial burden, resources, and regulations than some more classic agents such as fibrin clots. Fibrin clot is readily available, easy to use, affordable, and minimally invasive. This Technical Note describes a step-by-step and reproducible technique for harvesting, preparation, and using a fibrin clot to augment healing of meniscal repairs.
Figures


References
-
- Hede A., Larsen E., Sandberg H. The long term outcome of open total and partial meniscectomy related to the quantity and site of the meniscus removed. Int Orthop. 1992;16:122–125. - PubMed
-
- Verdonk R., Madry H., Shabshin N. The role of meniscal tissue in joint protection in early osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2016;24:1763–1774. - PubMed
-
- Parker B.R., Hurwitz S., Spang J., Creighton R., Kamath G. Surgical trends in the treatment of meniscal tears: Analysis of data from the American Board of Orthopaedic Surgery Certification Examination Database. Am J Sports Med. 2016;44:1717–1723. - PubMed
-
- Xu C., Zhao J. A meta-analysis comparing meniscal repair with meniscectomy in the treatment of meniscal tears: The more meniscus, the better outcome? Knee Surg Sports Traumatol Arthrosc. 2015;23:164–170. - PubMed
-
- Lutz C., Dalmay F., Ehkirch F.P., French Arthroscopy Society Meniscectomy versus meniscal repair: 10 years radiological and clinical results in vertical lesions in stable knee. Orthop Traumatol Surg Res. 2015;101(suppl):S327–S331. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
