

doi: 10.1016/j.eats.2017.08.018.
eCollection 2017 Dec.
Medial Patellofemoral Ligament Reconstruction Using Dual Patella Docking Technique
Affiliations
- PMID: 29349002
- PMCID: PMC5766319
- DOI: 10.1016/j.eats.2017.08.018
Item in Clipboard
Medial Patellofemoral Ligament Reconstruction Using Dual Patella Docking Technique
Arthrosc Tech.
.
Abstract
Medial patellofemoral ligament (MPFL) injuries are common in children and young adults. In patients with recurrent patellar dislocations with normal lower-extremity alignment, anatomic reconstruction of the MPFL has been shown to restore patellar stability. We describe a technique that creates an anatomic reconstruction using a dual docking technique into the patella. Our technique is simple and efficacious for reconstructing the MPFL without implant fixation in the patella, allowing a maximal bone-tendon interface for healing.
Figures

Graft preparation using Acufex tensioning device (Smith & Nephew). To the left is the single arm that will be inserted into the distal femur; to the right are the 2 arms that will be inserted into the patella.
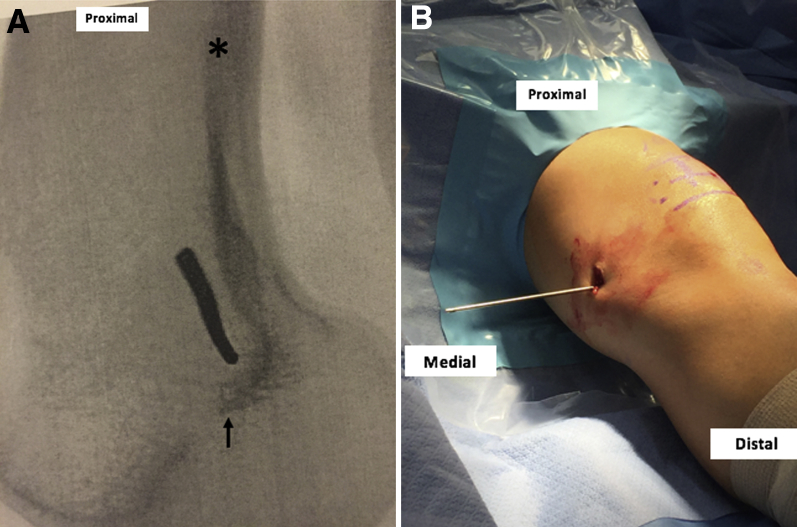
(A) Lateral radiograph of a knee with anterior to the left and posterior to the right with the pin at our femoral tunnel location, anterior to the posterior cortical line (asterisk) and superior to the Blumensaat line (arrow). (B) Clinical photograph of a left knee in a patient positioned supine with the Beath pin entering through a medial incision, drilled into the femoral tunnel starting location.

Photograph of a left knee in a patient positioned supine with proximal to the left and distal to the right. The semitendinosus graft (arrow) is being secured into the medial femoral tunnel. The guidewire (asterisk) for an interference screw is in place.

Photograph of a left knee in a patient positioned supine with proximal to the left and distal to the right. One limb of the semitendinosus graft (arrow) is being shuttled through the medial knee retinacular tunnel, exiting adjacent to the patella. The second limb (asterisk) has not yet been shuttled.

(A) Photograph of a left knee in a patient positioned supine with proximal to the left and distal to the right. The medial aspect of the patella with the 2 tunnel sites is marked (arrows). Two Beath pins are drilled through the patella at these sites. (B) Lateral fluoroscopic image of a left knee after the Beath pins (arrows) have been drilled from medial to lateral across the patella. The image confirms that the pins remain extra-articular as they cross the patella.

Photograph of a left knee in a patient positioned supine with proximal to the left and distal to the right. We prepare to drill our tunnel with a 4.0-mm cannulated reamer (asterisk). The reamer has been marked at 2 cm (arrow). We visually confirm that the spacing is adequate such that the tunnels do not meet.

Photographs of a left knee in a patient positioned supine with proximal to the left and distal to the right. (A) Measurement of graft limbs. We mark the graft 2 cm distal (arrowhead) to the point at which it makes contact with the medial cortex of the patella (arrow). (B) Suturing of grafts with a straight needle (asterisk) and a looped FiberWire suture from the point of contact with the medial cortex of the patella (arrow) to the marked point 2 cm distal (arrowhead).

(A) Photograph of a left knee in a patient positioned supine with proximal at the top and distal at the bottom. Both graft limbs have been secured into their respective patellar tunnels (asterisks) on the medial aspect of the patella. (B) Sutures coming out of the lateral incision after they have been passed through the patella from medial to lateral. The sutures from the different graft limbs are tied to each other.
Similar articles
-
Clinical outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent patella instability.Knee Surg Sports Traumatol Arthrosc. 2016 Mar;24(3):666-71. doi: 10.1007/s00167-014-3439-x. Epub 2014 Nov 22. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 25416673
-
The ability of medial patellofemoral ligament reconstruction to correct patellar kinematics and contact mechanics in the presence of a lateralized tibial tubercle.Am J Sports Med. 2015 Sep;43(9):2198-207. doi: 10.1177/0363546515597906. Epub 2015 Aug 19. Am J Sports Med. 2015. PMID: 26290576
-
Medial Patellofemoral Ligament Reconstruction Using All-Soft Suture Anchors for Patellar Fixation.Arthrosc Tech. 2018 Feb 12;7(3):e231-e237. doi: 10.1016/j.eats.2017.08.075. eCollection 2018 Mar. Arthrosc Tech. 2018. PMID: 29881694 Free PMC article.
-
Anatomic Double-Bundle Medial Patellofemoral Ligament Reconstruction with Autologous Semitendinosus: Aperture Fixation Both at the Femur and the Patella.Joints. 2017 Oct 4;5(4):256-260. doi: 10.1055/s-0037-1607192. eCollection 2017 Dec. Joints. 2017. PMID: 29270566 Free PMC article. Review.
-
Quadriceps Tendon Autograft Medial Patellofemoral Ligament Reconstruction.Curr Rev Musculoskelet Med. 2018 Jun;11(2):209-220. doi: 10.1007/s12178-018-9476-1. Curr Rev Musculoskelet Med. 2018. PMID: 29679209 Free PMC article. Review.
Cited by
-
Medial Patellofemoral Ligament Reconstruction: A Surgical Technique to Dynamically Control Graft Tension.Arthrosc Tech. 2022 Nov 18;11(12):e2309-e2318. doi: 10.1016/j.eats.2022.08.023. eCollection 2022 Dec. Arthrosc Tech. 2022. PMID: 36632405 Free PMC article.
-
Surgical Technique: Anatomic Medial Patellofemoral Ligament Retensioning Repair.Arthrosc Tech. 2018 Apr 30;7(5):e569-e574. doi: 10.1016/j.eats.2018.02.001. eCollection 2018 May. Arthrosc Tech. 2018. PMID: 29868436 Free PMC article.
-
Anatomic MPFL reconstruction with Gracillis autograft using all suture anchors.J Clin Orthop Trauma. 2025 Apr 17;66:103016. doi: 10.1016/j.jcot.2025.103016. eCollection 2025 Jul. J Clin Orthop Trauma. 2025. PMID: 40329932 No abstract available.
References
-
- Baldwin J.L. The anatomy of the medial patellofemoral ligament. Am J Sports Med. 2009;37:2355–2361. - PubMed
-
- Nomura E., Horiuchi Y., Kihara M. Medial patellofemoral ligament restraint in lateral patellar translation and reconstruction. Knee. 2000;7:121–127. - PubMed
-
- Amis A.A., Firer P., Mountney J., Senavongse W., Thomas N.P. Anatomy and biomechanics of the medial patellofemoral ligament. Knee. 2003;10:215–220. - PubMed
-
- Desio S.M., Burks R.T., Bachus K.N. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med. 1998;26:59–65. - PubMed
-
- Hautamaa P.V., Fithian D.C., Kaufman K.R., Daniel D.M., Pohlmeyer A.M. Medial soft tissue restraints in lateral patellar instability and repair. Clin Orthop Relat Res. 1998;(349):174–182. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
