

Learning fiberoptic intubation for awake nasotracheal intubation
- PMID: 29349352
- PMCID: PMC5766089
- DOI: 10.17245/jdapm.2017.17.4.297
Learning fiberoptic intubation for awake nasotracheal intubation
Abstract
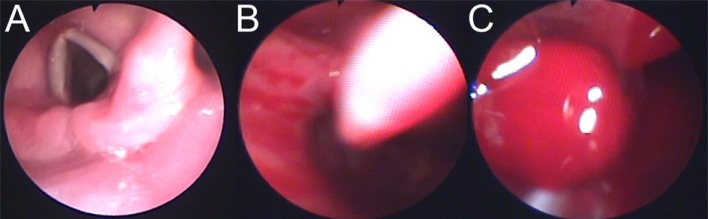
Background: Fiberoptic nasotracheal intubation (FNI) is performed if it is difficult to open the mouth or if intubation using laryngoscope is expected to be difficult. However, training is necessary because intubation performed by inexperienced operators leads to complications.
Methods: Every resident performed intubation in 40 patients. Success of FNI was evaluated as the time of FNI. First intubation time was restricted to 2 min 30 s. If the second attempt was unsuccessful, it was considered a failed case, and a specialist performed nasotracheal intubation. If the general method of intubation was expected to be difficult, awake intubation was performed. The degree of nasal bleeding during intubation was also evaluated.
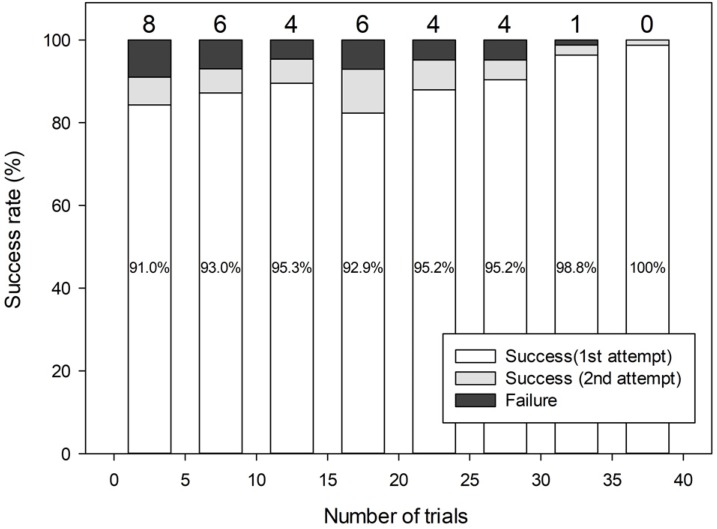
Results: The mean age of the operators (11 men, 7 women) was 27.8 years. FNI was performed in a total of 716 patients. The success rate was 88.3% for the first attempt and 94.6% for the second attempt. The failure rate of intubation in anesthetized patients was 4.9%, and 13.6% in awake patients. When intubation was performed in anesthetized patients, the failure rate from the first to fifth trial was 9.6%, which decreased to 0.7% when the number of trials increased to > 30 times. In terms of awake intubation, there was no failed attempt when the resident had performed the FNI > 30 times. The number of FNIs performed and nasal bleeding were important factors influencing the failure rate.
Conclusion: The success rate of FNI increased as the number of FNI performed by residents increased despite the nasal bleeding.
Keywords: Fiberscope; Learning curve; Nasotracheal intubation.
Conflict of interest statement
CONFLICTS OF INTEREST: The authors have no conflicts of interest to declare.
Figures



References
-
- Mahmood S, Lowe T. Management of epistaxis in the oral and maxillofacial surgery setting: An update on current practice. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:23–29. - PubMed
-
- Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG, et al. Practice guidelines for management of the difficult airway: An updated report by the american society of anesthesiologists task force on management of the difficult airway. Anesthesiology. 2013;118:251–270. - PubMed
-
- Delaney KA, Hessler R. Emergency flexible fiberoptic nasotracheal intubation: A report of 60 cases. Ann Emerg Med. 1988;17:919–926. - PubMed
-
- Ovassapian A, Yelich SJ, Dykes MH, Brunner EE. Fiberoptic nasotracheal intubation--incidence and causes of failure. Anesth Analg. 1983;62:692–695. - PubMed
-
- Smith JE, Jackson AP, Hurdley J, Clifton PJ. Learning curves for fibreoptic nasotracheal intubation when using the endoscopic video camera. Anaesthesia. 1997;52:101–106. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
