

Modern work-up and extended resection in perihilar cholangiocarcinoma: the AMC experience
- PMID: 29350267
- PMCID: PMC5986829
- DOI: 10.1007/s00423-018-1649-2
Modern work-up and extended resection in perihilar cholangiocarcinoma: the AMC experience
Abstract
Aim: Perihilar cholangiocarcinoma (PHC) is a challenging disease and requires aggressive surgical treatment in order to achieve curation. The assessment and work-up of patients with presumed PHC is multidisciplinary, complex and requires extensive experience. The aim of this paper is to review current aspects of diagnosis, preoperative work-up and extended resection in patients with PHC from the perspective of our own institutional experience with this complex tumor.
Methods: We provided a review of applied modalities in the diagnosis and work-up of PHC according to current literature. All patients with presumed PHC in our center between 2000 and 2016 were identified and described. The types of resection, surgical techniques and outcomes were analyzed.
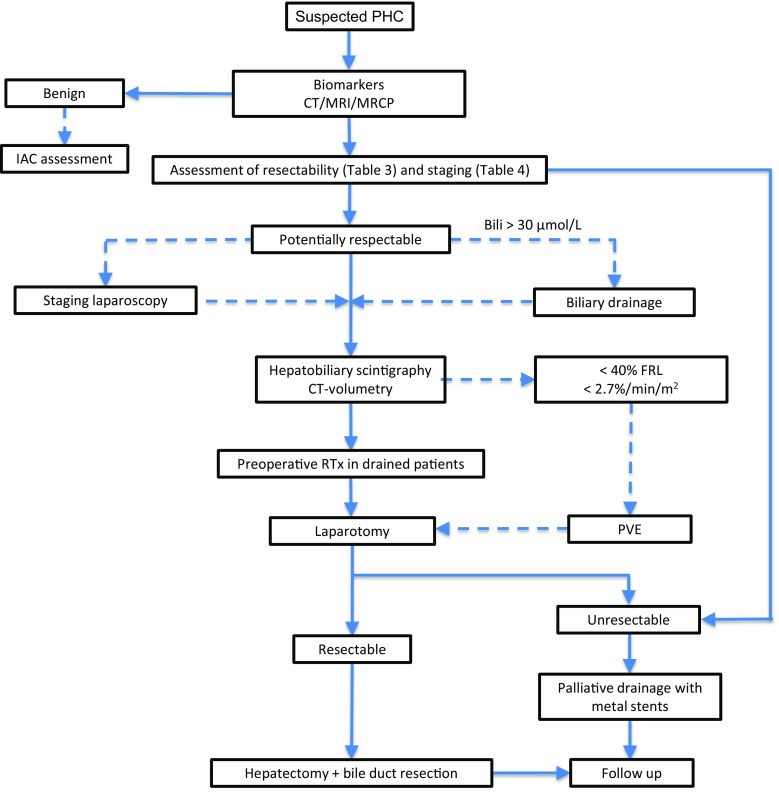
Results and conclusion: Upcoming diagnostic modalities such as Spyglass and combinations of serum biomarkers and molecular markers have potential to decrease the rate of misdiagnosis of benign, inflammatory disease. Assessment of liver function with hepatobiliary scintigraphy provides better information on the future remnant liver (FRL) than volume alone. The selective use of staging laparoscopy is advisable to avoid futile laparotomies. In patients requiring extended resection, selective preoperative biliary drainage is mandatory in cholangitis and when FRL is small (< 50%). Preoperative portal vein embolization (PVE) is used when FRL volume is less than 40% and optionally includes the left portal vein branches to segment 4. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) as alternative to PVE is not recommended in PHC. N2 positive lymph nodes preclude long-term survival. The benefit of unconditional en bloc resection of the portal vein bifurcation is uncertain. Along these lines, an aggressive surgical approach encompassing extended liver resection including segment 1, regional lymphadenectomy and conditional portal venous resection translates into favorable long-term survival.
Keywords: Biliary drainage; Biomarkers; Diagnosis; Hepato-biliary scintigraphy; Klatskin tumor; Perihilar cholangiocarcinoma; Postoperative outcome; Preoperative assessment; Staging; Surgical resection.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
