

Realizing the Mass Public Benefit of Evidence-Based Psychological Therapies: The IAPT Program
- PMID: 29350997
- PMCID: PMC5942544
- DOI: 10.1146/annurev-clinpsy-050817-084833
Realizing the Mass Public Benefit of Evidence-Based Psychological Therapies: The IAPT Program
Abstract
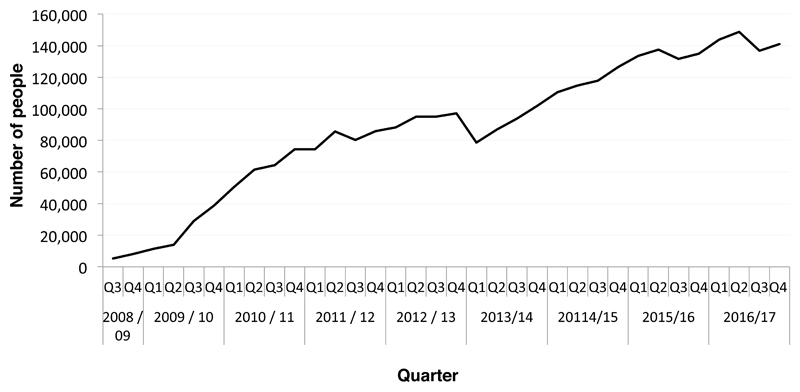
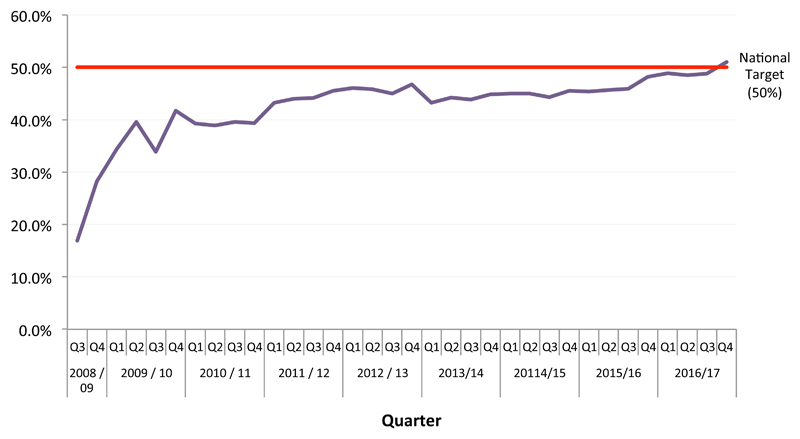
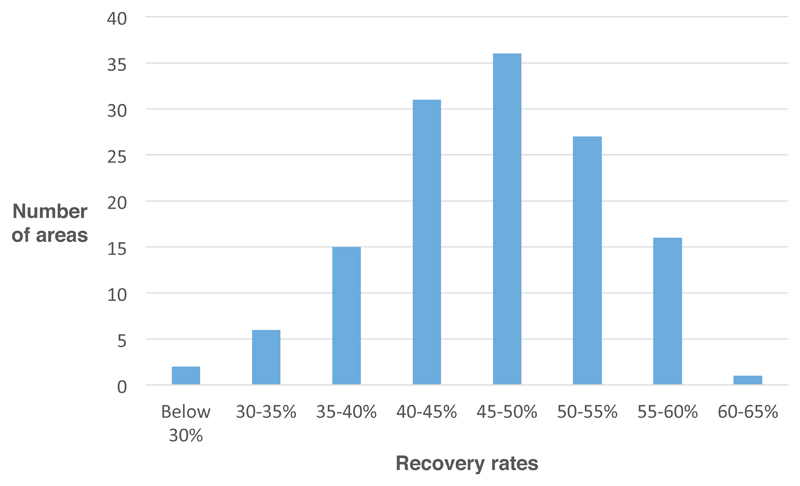
Empirically supported psychological therapies have been developed for many mental health conditions. However, in most countries only a small proportion of the public benefit from these advances. The English Improving Access to Psychological Therapies (IAPT) program aims to bridge the gap between research and practice by training over 10,500 new psychological therapists in empirically supported treatments and deploying them in new services for the treatment of depression and anxiety disorders. Currently IAPT treats over 560,000 patients per year, obtains clinical outcome data on 98.5% of these individuals, and places this information in the public domain. Around 50% of patients treated in IAPT services recover, and two-thirds show worthwhile benefits. The clinical and economic arguments on which IAPT is based are presented, along with details of the service model, how the program was implemented, and recent findings about service organization. Limitations and future directions are outlined.
Keywords: anxiety disorders; depression; dissemination; outcome monitoring; psychological therapies.
Figures
References
-
- Barkham M, Margison F, Leach C, Lucock M, Mellor-Clark J, et al. Service profiling and outcomes benchmarking using the CORE-OM: Toward practice-based evidence in the psychological therapies. J Consult Clin Psychol. 2001;69:184–96. - PubMed
-
- Blackburn IM, James IA, Milne DL, Baker C, Standart S, et al. The Revised Cognitive Therapy Scale (Cts-R): Psychometric Properties. Behav Cogn Psychother. 2001;29:431–46.
-
- Chambless DL, Caputo GC, Jasin SE, Gracely EJ, Williams C. The mobility inventory for agoraphobia. Behav Res Ther. 1985;23:35–44. - PubMed
-
- Clark DM, Canvin L, Green J, Layard R, Pilling S, Janecka M. Transparency about the outcomes of mental health services (IAPT approach): an analysis of public data. Lancet. 2017 doi: 10.1016/S0140-6736(17)32133-5. online pub December 7th. [publically available data is used to understand differences in outcome between IAPT services] - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
