

Angiography and Embolization in the Management of Bleeding Pelvic Fractures
- PMID: 29351135
- PMCID: PMC5794236
- DOI: 10.5435/JAAOS-D-16-00600
Angiography and Embolization in the Management of Bleeding Pelvic Fractures
Abstract
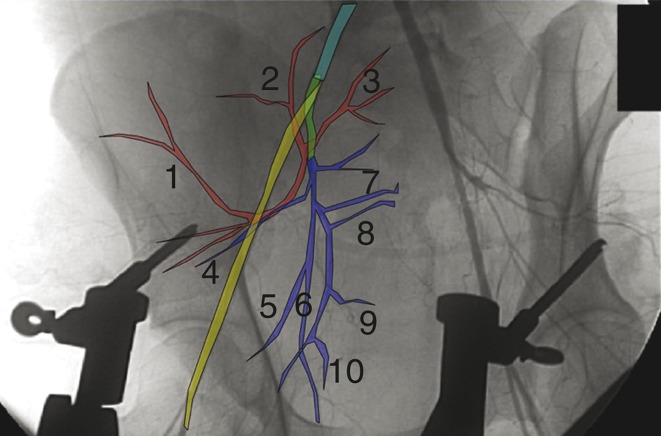
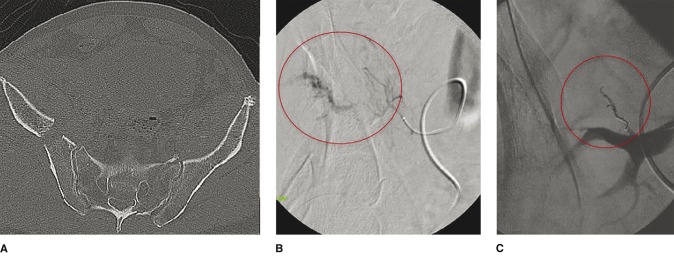
The use, timing, and priority of angioembolization in the management of bleeding pelvic fractures remain ambiguous. The most common vessels for angioembolization are, in decreasing order, the internal iliac artery and its branches, the superior gluteal artery, the obturator artery, and the internal pudendal artery. Technical success rates for this treatment option range from 74% to 100%. The fracture patterns most commonly requiring angioembolization are the Young and Burgess lateral compression and anterior-posterior compression types and Tile type C. Mortality rates after angioembolization of 16% to 50% have been reported, but deaths are usually related to concomitant injuries. The sensitivity and specificity of contrast-enhanced CT in detecting the need for angioembolization range from 60% to 90% and 92% to 100%, respectively. Angioembolization can be effective in the management of bleeding pelvic fractures, but as with any treatment, the risks of complications must be considered. Availability of angioembolization and institutional expertise/preference for the alternative strategy of pelvic packing influence its use.
Figures
References
-
- Durkin A, Sagi HC, Durham R, Flint L: Contemporary management of pelvic fractures. Am J Surg 2006;192(2):211-223. - PubMed
-
- Costantini TW, Bosarge PL, Fortlage D, Bansal V, Coimbra R: Arterial embolization for pelvic fractures after blunt trauma: Are we all talk? Am J Surg 2010;200(6):752-758. - PubMed
-
- Magnussen RA, Tressler MA, Obremskey WT, Kregor PJ: Predicting blood loss in isolated pelvic and acetabular high-energy trauma. J Orthop Trauma 2007;21(9):603-607. - PubMed
-
- El-Haj M, Bloom A, Mosheiff R, Liebergall M, Weil YA: Outcome of angiographic embolisation for unstable pelvic ring injuries: Factors predicting success. Injury 2013;44(12):1750-1755. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
