

Effects of a population-based, person-centred and integrated care service on health, wellbeing and self-management of community-living older adults: A randomised controlled trial on Embrace
- PMID: 29351295
- PMCID: PMC5774687
- DOI: 10.1371/journal.pone.0190751
Effects of a population-based, person-centred and integrated care service on health, wellbeing and self-management of community-living older adults: A randomised controlled trial on Embrace
Abstract
Objective: To evaluate the effects of the population-based, person-centred and integrated care service 'Embrace' at twelve months on three domains comprising health, wellbeing and self-management among community-living older people.
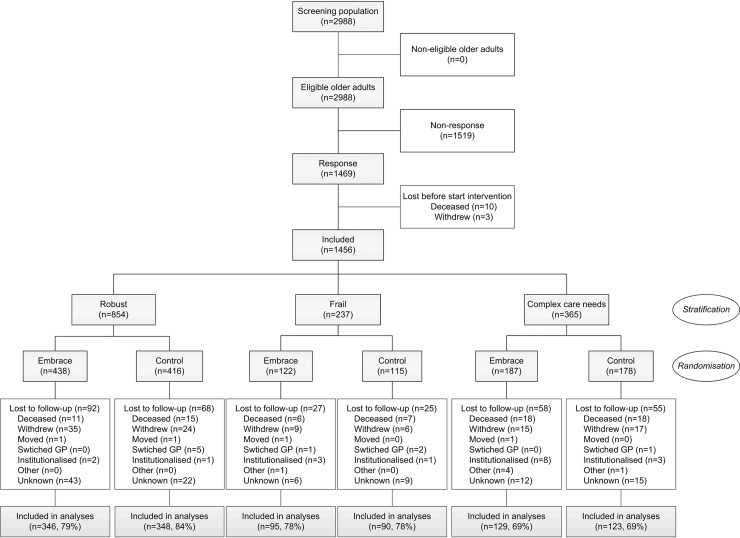
Methods: Embrace supports older adults to age in place. A multidisciplinary team provides care and support, with intensity depending on the older adults' risk profile. A randomised controlled trial was conducted in fifteen general practices in the Netherlands. Older adults (≥75 years) were included and stratified into three risk profiles: Robust, Frail and Complex care needs, and randomised to Embrace or care as usual (CAU). Outcomes were recorded in three domains. The EuroQol-5D-3L and visual analogue scale, INTERMED for the Elderly Self-Assessment, Groningen Frailty Indicator and Katz-15 were used for the domain 'Health.' The Groningen Well-being Indicator and two quality of life questions measured 'Wellbeing.' The Self-Management Ability Scale and Partners in Health scale for older adults (PIH-OA) were used for 'Self-management.' Primary and secondary outcome measurements differed per risk profile. Data were analysed with multilevel mixed-model techniques using intention-to-treat and complete case analyses, for the whole sample and per risk profile.
Results: 1456 eligible older adults participated (49%) and were randomized to Embrace (n(T0) = 747, n(T1) = 570, mean age 80.6 years (SD 4.5), 54.2% female) and CAU (n(T0) = 709, n(T1) = 561, mean age 80.8 years (SD 4.7), 55.6% female). Embrace participants showed a greater-but clinically irrelevant-improvement in self-management (PIH-OA Knowledge subscale effect size [ES] = 0.14), and a greater-but clinically relevant-deterioration in health (ADL ES = 0.10; physical ADL ES = 0.13) compared to CAU. No differences in change in wellbeing were observed. This picture was also found in the risk profiles. Complete case analyses showed comparable results.
Conclusions: This study found no clear benefits to receiving person-centred and integrated care for twelve months for the domains of health, wellbeing and self-management in community-living older adults.
Conflict of interest statement
Figures
References
-
- Sixsmith J, Sixsmith A, Fange AM, Naumann D, Kucsera C, Tomsone S, et al. Healthy ageing and home: the perspectives of very old people in five European countries. Soc Sci Med. 2014;106: 1–9. doi: 10.1016/j.socscimed.2014.01.006 - DOI - PubMed
-
- Lofqvist C, Granbom M, Himmelsbach I, Iwarsson S, Oswald F, Haak M. Voices on relocation and aging in place in very old age—a complex and ambivalent matter. Gerontologist. 2013;53: 919–927. doi: 10.1093/geront/gnt034 - DOI - PubMed
-
- Wiles JL, Leibing A, Guberman N, Reeve J, Allen RE. The meaning of "aging in place" to older people. Gerontologist. 2012;52: 357–366. doi: 10.1093/geront/gnr098 - DOI - PubMed
-
- Spoorenberg SL, Reijneveld SA, Middel B, Uittenbroek RJ, Kremer HP, Wynia K. The Geriatric ICF Core Set reflecting health-related problems in community-living older adults aged 75 years and older without dementia: development and validation. Disabil Rehabil. 2015;37: 2337–2343. doi: 10.3109/09638288.2015.1024337 - DOI - PubMed
-
- Chen Y, Feeley TH. Social support, social strain, loneliness, and well-being among older adults: an analysis of the Health and Retirement Study. JSPR. 2014;31: 141.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
