

Prognostic relevance of elevated pulmonary arterial pressure assessed non-invasively: Analysis in a large patient cohort with invasive measurements in near temporal proximity
- PMID: 29351312
- PMCID: PMC5774714
- DOI: 10.1371/journal.pone.0191206
Prognostic relevance of elevated pulmonary arterial pressure assessed non-invasively: Analysis in a large patient cohort with invasive measurements in near temporal proximity
Abstract
Background: The clinical relevance of non-invasively derived pulmonary arterial pressure (PAP) by Doppler echocardiography (DE) has been questioned in the past. However, transthoracic echocardiography is used as a cornerstone examination for patients with dyspnea and suspected pulmonary hypertension (PH). This study aimed to evaluate the prognostic value of non-invasive assessed PAP in a large population of patients with known or suspected cardiopulmonary disease.
Methods: The analyses are based on data of patients of a tertiary cardiology center that received right heart catheterization (RHC) as well as non-invasively assessed PAP by DE within five days, and includes serological and clinical parameters in a retrospective follow-up for up to eight years.
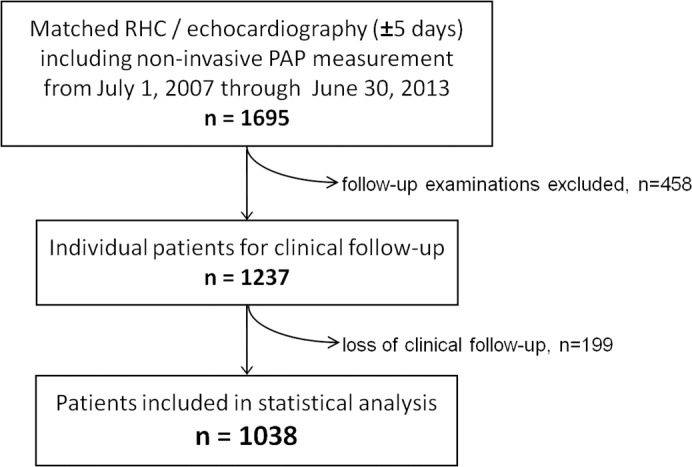
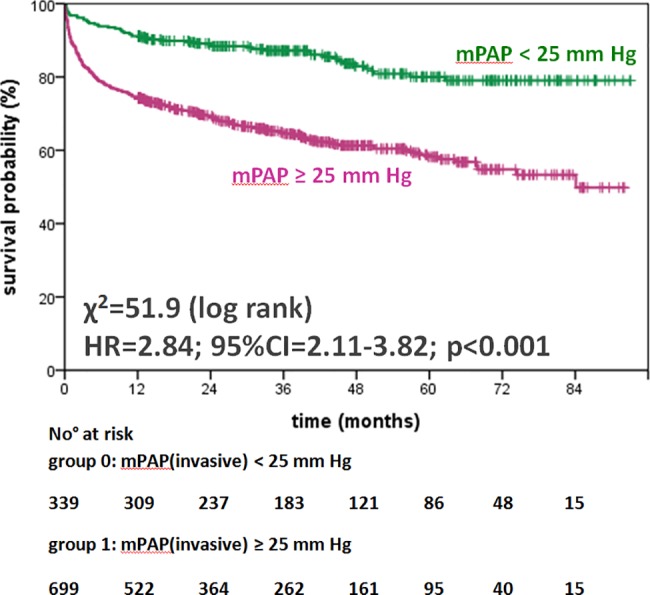
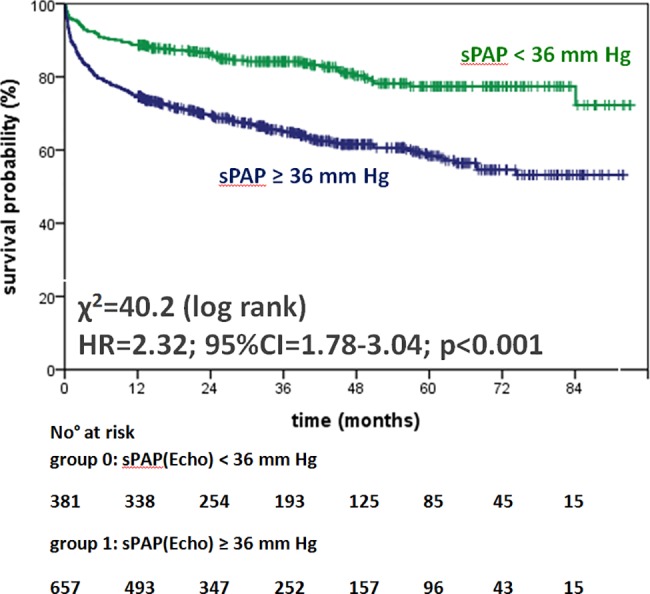
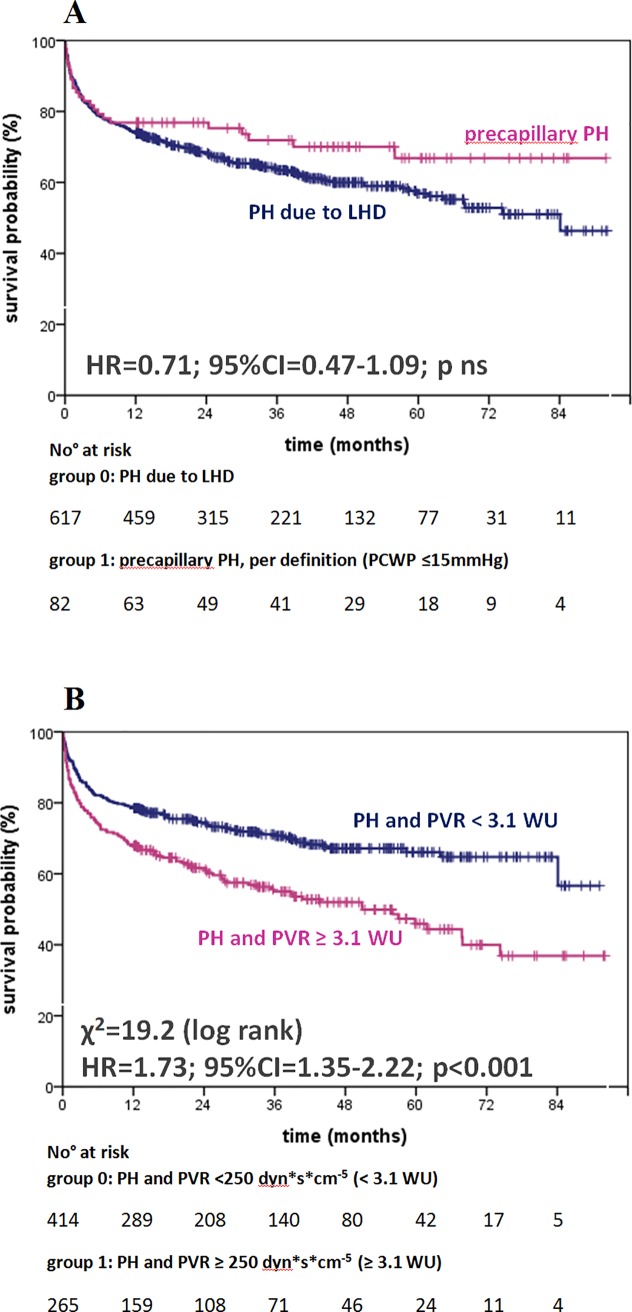
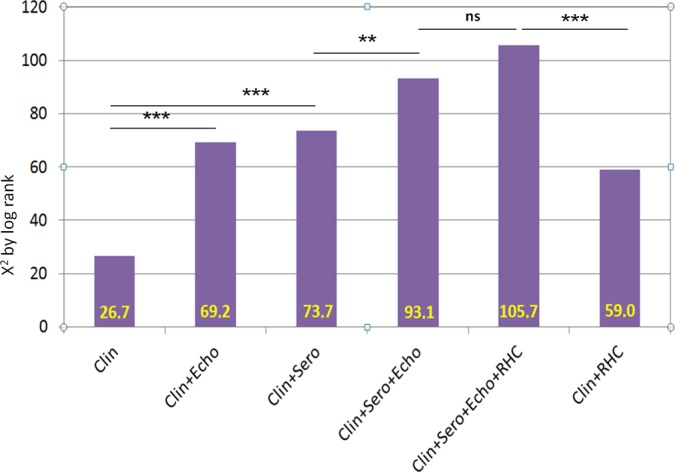
Results: Of 1,237 patients, clinical follow-up was possible in 1,038 patients who were included in the statistical analysis. The mean-follow up time was 1,002 days. The composite endpoint of heart transplantation (HTx) or death occurred in n = 308 patients. Elevated PAP measured non-invasively as well as invasively had significant prognostic impact (hazard ratio (HR) 2.32; 95% confidence interval (CI) 1.78-3.04; χ2 = 37.9; p<0.001 versus HR 2.84; 95%CI 2.11-3.82; χ2 = 51.9; p<0.001, respectively). By multivariate analysis, NYHA functional class, N-terminal pro-brain natriuretic peptide, cardiac troponin T, left ventricular ejection fraction, and right ventricular dysfunction remained independently predictive. Incremental prognostic information in a multimodal approach was highly relevant.
Conclusions: In this comprehensive study, elevated pulmonary arterial pressure measured by DE offers similar prognostic information on survival or need for HTx as right heart catheterization. Furthermore, the addition of functional capacity and serological biomarkers delivered incremental prognostic information.
Conflict of interest statement
Figures
Similar articles
-
Reliability of noninvasive assessment of systolic pulmonary artery pressure by Doppler echocardiography compared to right heart catheterization: analysis in a large patient population.J Am Heart Assoc. 2014 Aug 21;3(4):e001103. doi: 10.1161/JAHA.114.001103. J Am Heart Assoc. 2014. PMID: 25146706 Free PMC article.
-
Right atrial emptying fraction non-invasively predicts mortality in pulmonary hypertension.Int J Cardiovasc Imaging. 2016 Jul;32(7):1121-30. doi: 10.1007/s10554-016-0883-3. Epub 2016 Apr 13. Int J Cardiovasc Imaging. 2016. PMID: 27076226
-
[Echocardiography and right heart catheterization in pulmonal hypertension].Dtsch Med Wochenschr. 2014 Jul;139(30):1511-7. doi: 10.1055/s-0034-1370161. Epub 2014 Jul 29. Dtsch Med Wochenschr. 2014. PMID: 25072860 German.
-
Mild Pulmonary Hypertension Is Associated With Increased Mortality: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2018 Sep 18;7(18):e009729. doi: 10.1161/JAHA.118.009729. J Am Heart Assoc. 2018. PMID: 30371195 Free PMC article.
-
A diagnostic algorithm for pulmonary hypertension due to left heart disease in resource-limited settings: can busy clinicians adopt a simple, practical approach?Cardiovasc J Afr. 2019 Jan/Feb 23;30(1):61-67. doi: 10.5830/CVJA-2018-042. Epub 2018 Nov 30. Cardiovasc J Afr. 2019. PMID: 30534850 Review.
Cited by
-
PASCAL-based mitral valve repair in an all-comer population: acute and mid-term clinical results.ESC Heart Fail. 2021 Oct;8(5):3530-3538. doi: 10.1002/ehf2.13569. Epub 2021 Aug 27. ESC Heart Fail. 2021. PMID: 34448541 Free PMC article.
-
Systolic pulmonary artery pressure assessed during routine exercise Doppler echocardiography: insights of a real-world setting in patients with elevated pulmonary pressures.Int J Cardiovasc Imaging. 2018 Aug;34(8):1215-1225. doi: 10.1007/s10554-018-1340-2. Epub 2018 Mar 19. Int J Cardiovasc Imaging. 2018. PMID: 29552698
-
Prognostic relevance of the right ventricular myo-mechanical index (RV-MMI) in patients with precapillary pulmonary hypertension.Open Heart. 2018 Sep 12;5(2):e000903. doi: 10.1136/openhrt-2018-000903. eCollection 2018. Open Heart. 2018. PMID: 30245839 Free PMC article.
References
-
- Galiè N, Simonneau G. The Fifth World Symposium on Pulmonary Hypertension. J Am Coll Cardiol. 2013; 62: D1–3. doi: 10.1016/j.jacc.2013.10.030 - DOI - PubMed
-
- Vachiery J-L, Adir Y, Barberà JA, Champion H, Coghlan JG, Cottin V, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol. 2013; 62: D100–8. doi: 10.1016/j.jacc.2013.10.033 - DOI - PubMed
-
- Carbone R, Bossone E, Bottino G, Monselise A, Rubenfire M. Diagnosis and assessment of pulmonary arterial hypertension. Eur Rev Med Pharmacol Sci. 2005; 9: 331–42. - PubMed
-
- Badesch DB, Champion HC, Sanchez MA, Hoeper MM, Loyd JE, Manes A, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009; 54: S55–66. doi: 10.1016/j.jacc.2009.04.011 - DOI - PubMed
-
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010; 23: 685–713. doi: 10.1016/j.echo.2010.05.010 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
