

A novel risk classification system for 30-day mortality in children undergoing surgery
- PMID: 29351327
- PMCID: PMC5774754
- DOI: 10.1371/journal.pone.0191176
A novel risk classification system for 30-day mortality in children undergoing surgery
Abstract
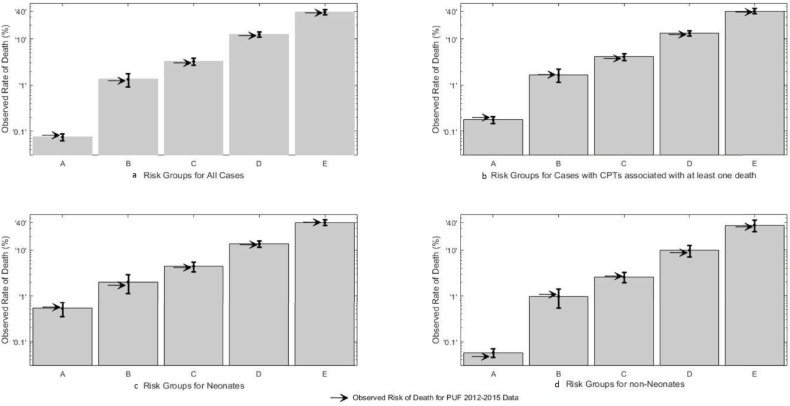
A simple, objective and accurate way of grouping children undergoing surgery into clinically relevant risk groups is needed. The purpose of this study, is to develop and validate a preoperative risk classification system for postsurgical 30-day mortality for children undergoing a wide variety of operations. The National Surgical Quality Improvement Project-Pediatric participant use file data for calendar years 2012-2014 was analyzed to determine preoperative variables most associated with death within 30 days of operation (D30). Risk groups were created using classification tree analysis based on these preoperative variables. The resulting risk groups were validated using 2015 data, and applied to neonates and higher risk CPT codes to determine validity in high-risk subpopulations. A five-level risk classification was found to be most accurate. The preoperative need for ventilation, oxygen support, inotropic support, sepsis, the need for emergent surgery and a do not resuscitate order defined non-overlapping groups with observed rates of D30 that vary from 0.075% (Very Low Risk) to 38.6% (Very High Risk). When CPT codes where death was never observed are eliminated or when the system is applied to neonates, the groupings remained predictive of death in an ordinal manner.
Conflict of interest statement
Figures
References
-
- Grosfeld JL and O’Neill JA Jr. History of Pediatric Surgery: A Brief Overview In: Coran AG, Adzick NS, Krummel TM, Laberge JM, Shamberger RC, Caldamone AA., editors. Pediatric Surgery, 7th Edition, Elsevier, Philadelphia, PA, 2012, p3–17.
-
- Semel ME, Lipsitz SR, Funk LM, Bader AM, Weiser TG, Gwande AA. Rates and patterns of death after surgery in the United States, 1996 and 2006. Surgery 2012; 151(2): 171–82. doi: 10.1016/j.surg.2011.07.021 - DOI - PubMed
-
- American College of Surgeons, https://www.facs.org/quality%20programs/pediatric/overview, [accessed 26.14.2016]
-
- Kraemer K, Cohen ME, Liu Y, Barnhart DC, Rangel SJ, Saito JM, Bilimoria KY, Ko CY, Hall BL. Development and evaluation of the American College of Surgeons NSQIP Pediatric surgical risk calculator. J Am Coll Surg. 2016; 223(5):685–93. doi: 10.1016/j.jamcollsurg.2016.08.542 - DOI - PubMed
-
- Optimal resources for Children’s Surgical Care 2015 Manual, American College of Surgeons, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
