

Tracheal intubation in critically ill patients: a comprehensive systematic review of randomized trials
- PMID: 29351759
- PMCID: PMC5775615
- DOI: 10.1186/s13054-017-1927-3
Tracheal intubation in critically ill patients: a comprehensive systematic review of randomized trials
Erratum in
-
Correction to: Tracheal intubation in critically ill patients: a comprehensive systematic review of randomized trials.Crit Care. 2019 Oct 21;23(1):325. doi: 10.1186/s13054-019-2634-z. Crit Care. 2019. PMID: 31639036 Free PMC article.
Abstract
Background: We performed a systematic review of randomized controlled studies evaluating any drug, technique or device aimed at improving the success rate or safety of tracheal intubation in the critically ill.
Methods: We searched PubMed, BioMed Central, Embase and the Cochrane Central Register of Clinical Trials and references of retrieved articles. Finally, pertinent reviews were also scanned to detect further studies until May 2017. The following inclusion criteria were considered: tracheal intubation in adult critically ill patients; randomized controlled trial; study performed in Intensive Care Unit, Emergency Department or ordinary ward; and work published in the last 20 years. Exclusion criteria were pre-hospital or operating theatre settings and simulation-based studies. Two investigators selected studies for the final analysis. Extracted data included first author, publication year, characteristics of patients and clinical settings, intervention details, comparators and relevant outcomes. The risk of bias was assessed with the Cochrane Collaboration's Risk of Bias tool.
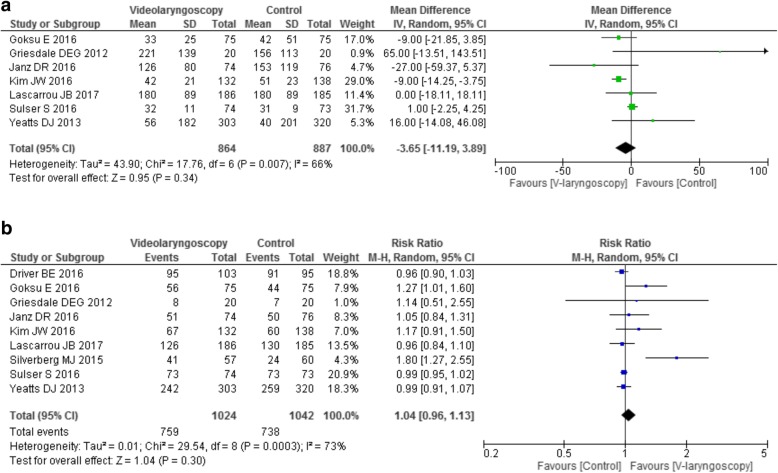
Results: We identified 22 trials on use of a pre-procedure check-list (1 study), pre-oxygenation or apneic oxygenation (6 studies), sedatives (3 studies), neuromuscular blocking agents (1 study), patient positioning (1 study), video laryngoscopy (9 studies), and post-intubation lung recruitment (1 study). Pre-oxygenation with non-invasive ventilation (NIV) and/or high-flow nasal cannula (HFNC) showed a possible beneficial role. Post-intubation recruitment improved oxygenation, while ramped position increased the number of intubation attempts and thiopental had negative hemodynamic effects. No effect was found for use of a checklist, apneic oxygenation (on oxygenation and hemodynamics), videolaryngoscopy (on number and length of intubation attempts), sedatives and neuromuscular blockers (on hemodynamics). Finally, videolaryngoscopy was associated with severe adverse effects in multiple trials.
Conclusions: The limited available evidence supports a beneficial role of pre-oxygenation with NIV and HFNC before intubation of critically ill patients. Recruitment maneuvers may increase post-intubation oxygenation. Ramped position increased the number of intubation attempts; thiopental had negative hemodynamic effects and videolaryngoscopy might favor adverse events.
Keywords: Critically ill; Emergency department; High flow nasal cannula; Intensive care unit; Tracheal intubation; Videolaryngoscopy.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
Comment in
-
Ramped position, an uncertain future.Crit Care. 2018 May 13;22(1):129. doi: 10.1186/s13054-018-2045-6. Crit Care. 2018. PMID: 29753330 Free PMC article. No abstract available.
References
-
- Jaber S, Amraoui J, Lefrant J-Y, Arich C, Cohendy R, Landreau L, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34:2355–61. - PubMed
-
- Jaber S, Jung B, Corne P, Sebbane M, Muller L, Chanques G, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010;36:248–55. - PubMed
-
- Simpson GD, Ross MJ, McKeown DW, Ray DC. Tracheal intubation in the critically ill: a multi-centre national study of practice and complications. Br J Anaesth. 2012;108:792–9. - PubMed
-
- Griesdale DEG, Bosma TL, Kurth T, Isac G, Chittock DR. Complications of endotracheal intubation in the critically ill. Intensive Care Med. 2008;34:1835–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
