

Clinical Pharmacokinetics and Pharmacodynamics of Evolocumab, a PCSK9 Inhibitor
- PMID: 29353350
- PMCID: PMC5999140
- DOI: 10.1007/s40262-017-0620-7
Clinical Pharmacokinetics and Pharmacodynamics of Evolocumab, a PCSK9 Inhibitor
Abstract
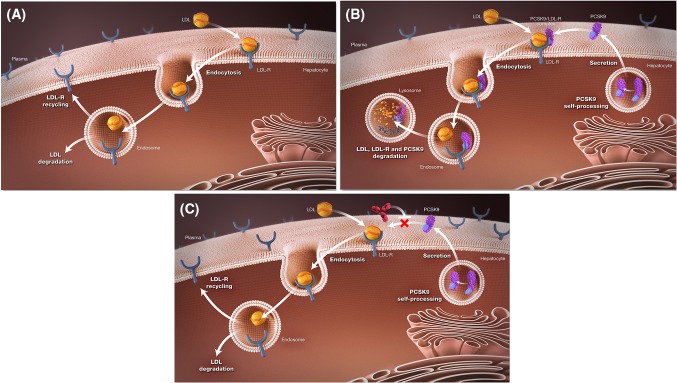
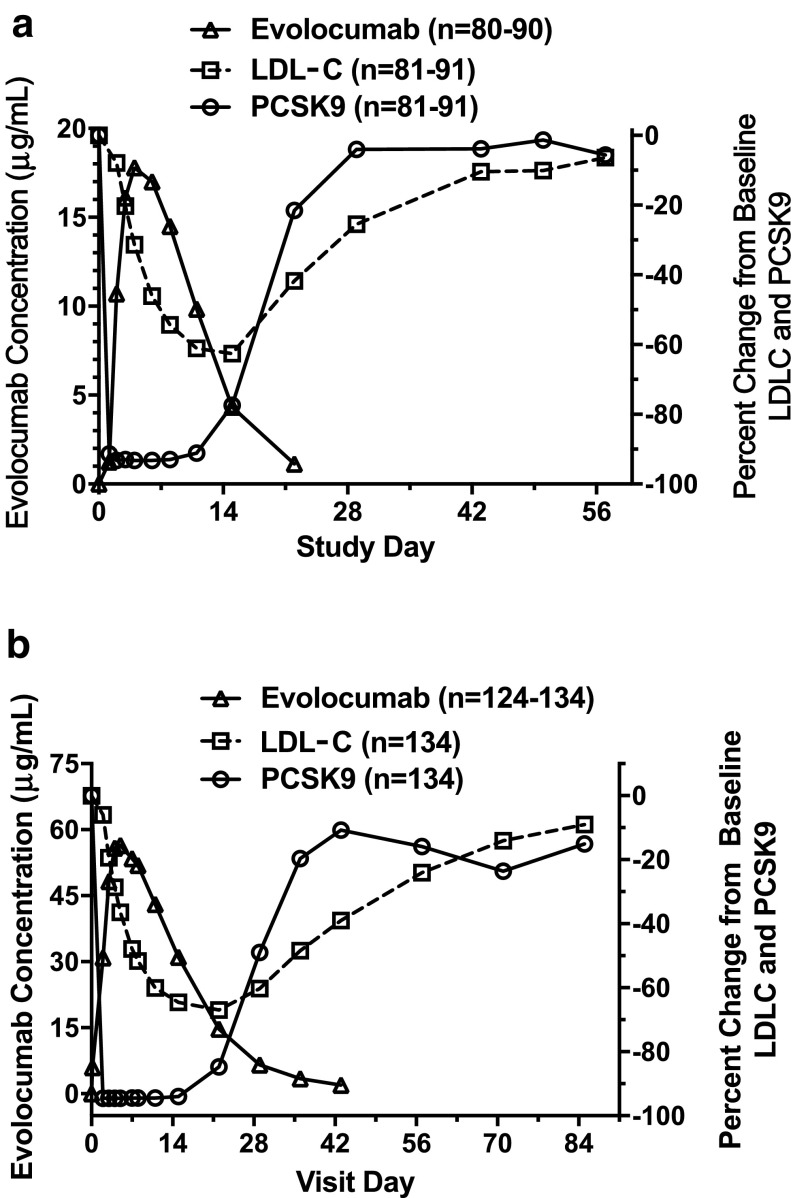
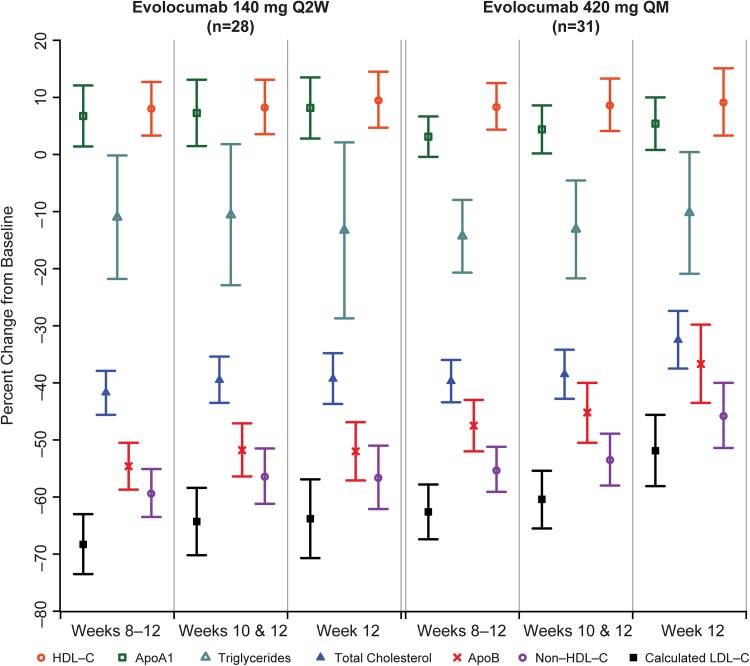
Proprotein convertase subtilisin/kexin type 9 (PCSK9) increases plasma low-density lipoprotein cholesterol (LDL-C) by decreasing expression of the LDL receptor on hepatic cells. Evolocumab is a human monoclonal immunoglobulin G2 that binds specifically to human PCSK9 to reduce LDL-C. Evolocumab exhibits nonlinear kinetics as a result of binding to PCSK9. Elimination is predominantly through saturable binding to PCSK9 at lower concentrations and a nonsaturable proteolytic pathway at higher concentrations. The effective half-life of evolocumab is 11-17 days. The pharmacodynamic effects of evolocumab on PCSK9 are rapid, with maximum suppression within 4 h. At steady state, peak reduction of LDL-C occurs approximately 1 week after a subcutaneous dose of 140 mg every 2 weeks (Q2W) and 2 weeks after a subcutaneous dose 420 mg once monthly (QM), and returns towards baseline over the dosing interval. In several clinical studies, these doses of evolocumab reduced LDL-C by approximately 55-75% compared with placebo. Evolocumab also reduced lipoprotein(a) [Lp(a)] levels and improved those of other lipids in clinical studies. No clinically meaningful differences in pharmacodynamic effects on LDL-C were observed in adult subjects regardless of mild/moderate hepatic impairment, renal impairment or renal failure, body weight, race, sex, or age. No clinically meaningful differences were observed for the pharmacodynamic effects of evolocumab on LDL-C between patients who received evolocumab alone or in combination with a statin, resulting in additional lowering of LDL-C when evolocumab was combined with a statin. No dose adjustment is necessary based on patient-specific factors or concomitant medication use.
Conflict of interest statement
Funding
This work was supported by Amgen Inc.
Conflict of interest
Drs. Somaratne and Wasserman are employees of and stockholders in Amgen, Inc. Drs. Somaratne and J.P. Gibbs are identified as inventors on at least one pending patent application owned by Amgen, Inc. relating to evolocumab. Dr. Wasserman appears on a number of pending patents owned by Amgen Inc. relating to evolocumab and PCSK9 inhibition. Drs. Kasichayanula, Grover, Emery, M. Gibbs, and J.P. Gibbs were employees of and stockholders in Amgen at the time this work was completed. Drs. Kasichayanula, M. Gibbs, and J.P. Gibbs are currently employed by AbbVie, Inc. Dr. Grover is currently employed by BioMarin Pharmaceutical Inc. Dr. Emery is currently employed by Seattle Genetics.
Figures
References
-
- World Health Organization . World health statistics 2012. Geneva: WHO Press; 2012.
-
- Collaboration Cholesterol Treatment Trialists, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi: 10.1016/S0140-6736(10)61350-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
