

doi: 10.5114/kitp.2017.72234.
Epub 2017 Dec 20.
Heart transplantation in the treatment of primary non-operable cardiac tumors
Affiliations
- PMID: 29354182
- PMCID: PMC5767780
- DOI: 10.5114/kitp.2017.72234
Item in Clipboard
Heart transplantation in the treatment of primary non-operable cardiac tumors
Kardiochir Torakochirurgia Pol.
2017 Dec.
No abstract available
Figures
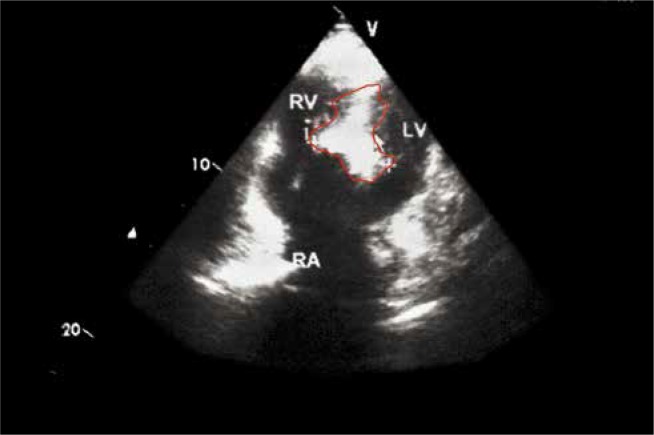
Tumor of interventricular septum and right ventricle of 40/20 mm (EchoCG dated 2009). The visible part of the tumor is demarked by a red line RV – right ventricle, RA – right atrium, LV – left ventricle

Gross specimen of the recipient heart containing benign tumor (leiomyoma) on the cross-sectioned surface: tumor is indicated by asterisk RV – right ventricle, LV – left ventricle

Recipient heart tumor pathology study: leiomyoma: A – Thin strip of RV myocardium on the right side of the figure. The tumor has severe spreading secondary changes: sclerosis and small foci of calcification. H + E, 1.25× objective. B – The tumor is represented by fibers and cells with regular elongated nuclei without polymorphism, with α-SMA-positive immunohistochemistry. H + E, 1.25× objective
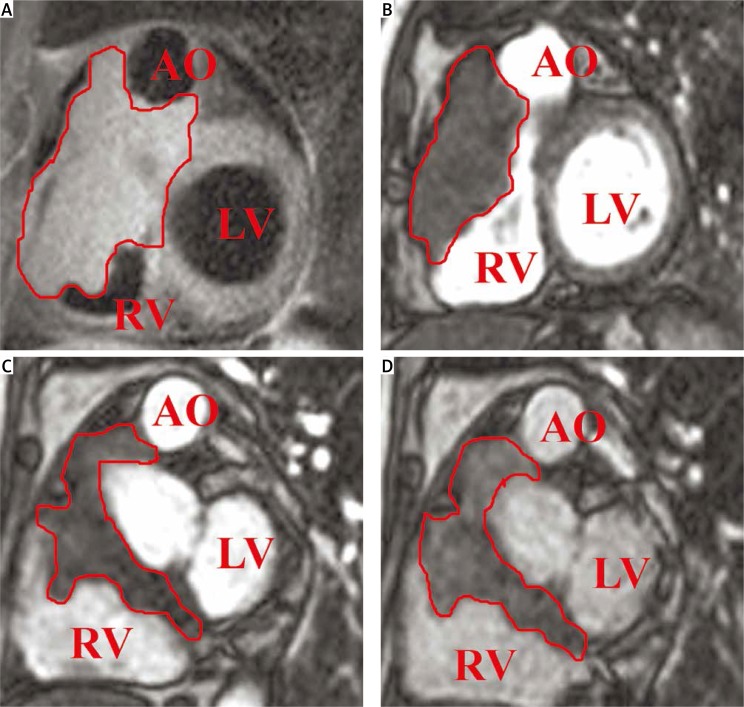
Right ventricle tumor spreading to right and left atrium, and to aortic root (MRI) LV – left ventricle, AO – aorta, RV – right ventricle

Orthotopic heart transplantation steps in patient with primary non-respectable malignant tumor of the heart: A – heart tumor revision after sternotomy. The visible part of the tumor is demarked by a white line. B – Explantation of the recipient heart with tumor. C – Reconstruction of neo-atrium using xenopericardium. D – Completion of orthotopic heart transplantation RA – right atrium, AO – aorta

Results of stent placement in the anastomotic area between vena cava inferior and right atrium – patency in the stenosis area was restored (cavography): stent is shown by the arrow

Pathology study of the recipient heart, affected by lymphoma: A – gross specimen of the recipient heart – tumor is demarked by a white line. B – Mitral valve damaged by lymphoma (asterisk). C – Fixed gross specimen of the heart (cross-section under the line of atrioventricular valves fibrous rings). Tumor (asterisk) presented by white foci replaces the myocardium of the right ventricle, invades epicardium, grows around coronary arteries, diffusely spreading in the myocardium of the left ventricle (LV). D – Microscopic picture of large B-cell lymphoma of the heart. Tumor replaces the myocardium and invades interstitium between muscle cells; tumor is presented by solid areas containing polymorphic round cells with positive immunohistochemistry for CD 20. 200× objective, H + E staining

Autopsy results: A – donor heart with repaired left atrium using xenopericardium patch. Patch is shown by arrow. B and C – Patency of anastomosis between IVC and RA of the donor hear in the area of stent placement, stent is shown by arrow. D – Extensive haemodynamic necrosis (yellow areas – arrow)
References
-
- Centofanti P, Di Rosa E, Deorsola L, Dato GM, Patanè F, La Torre M, Barbato L, Verzini A, Fortunato G, di Summa M. Primary cardiac tumors: early and late results of surgical treatment in 91 patients. Ann Thorac Surg. 1999;68:1236–1241. - PubMed
-
- Kamiya H, Yasuda T, Nagamine H, Sakakibara N, Nishida S, Kawasuji M, Watanabe G. Surgical treatment of primary cardiac tumors – 28 years’ experience in Kanazawa University Hospital. Jpn Circ J. 2001;65:315–319. - PubMed
-
- Piazza N, Chughtai T, Toledano K, Sampalis J, Liao C, Morin JF. Primary cardiac tumours: eighteen years of surgical experience on 21 patients. Can J Cardiol. 2004;20:1443–1448. - PubMed
-
- Dein JR, Frist WH, Stinson EB, Miller DC, Baldwin JC, Oyer PE, Jamieson S, Mitchell RS, Shumway NE. Primary cardiac neoplasms: early and late results of surgical treatment in 42 patients. J Thorac Cardiovasc Surg. 1987;93:502–511. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources