

Review
doi: 10.17096/jiufd.27242.
eCollection 2017.
Imaging evaluation of trigeminal neuralgia
Affiliations
- PMID: 29354310
- PMCID: PMC5750829
- DOI: 10.17096/jiufd.27242
Item in Clipboard
Review
Imaging evaluation of trigeminal neuralgia
J Istanb Univ Fac Dent.
.
Abstract
Trigeminal neuralgia is a debilitating pain syndrome in the sensory distribution of the trigeminal nerve. Compression of the cisternal segment of the trigeminal nerve by a vessel, usually an artery, is considered the most common cause of trigeminal neuralgia. A number of additional lesions may affect the trigeminal nerve anywhere along its course from the trigeminal nuclei to the most peripheral branches to cause facial pain. Relevant differential considerations are reviewed starting proximally at the level of the brainstem.
Keywords: magnetic resonance imaging; Trigeminal neuralgia; brainstem; facial pain; neurovascular conflict.
Conflict of interest statement
Conflict of interest: None declared.
Figures
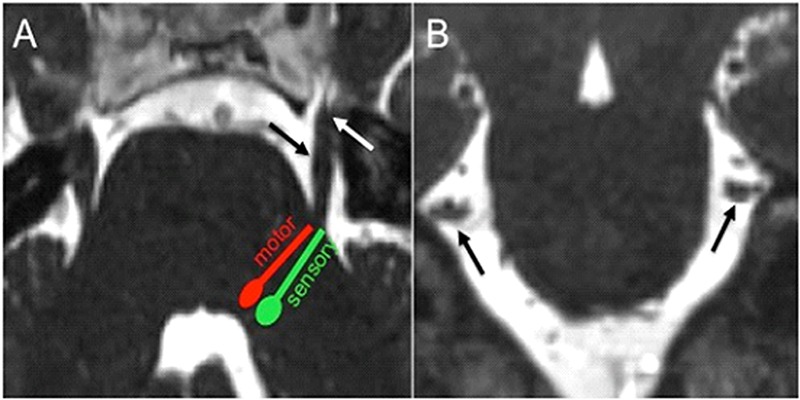
(a) Axial CISS image demonstrates the approximate location of the pontine trigeminal nuclei with their fibers projecting
towards the anterolateral aspect of the pons to form the cisternal segment of CN V (black arrow), which extends anteriorly to enter the
Meckel’s cave through the porus trigeminus (white arrow). (b) Coronal CISS image shows the cisternal segment of CN bilaterally in
cross section (black arrows). Coronal reconstructions are helpful for evaluation of neurovascular conflict.
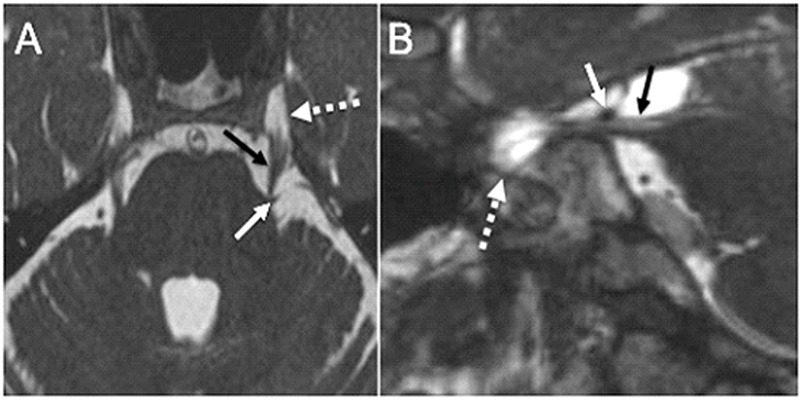
Neurovascular conflict causing TN. (a) Axial CISS image shows a vascular loop (white arrow), the left superior cerebellar
artery, mildly deforming the root entry zone of the cisternal segment of the left CN V (black arrow). Note the cisternal segment bilaterally
extending anteriorly to enter the Meckel’s cave (dashed arrow), which is filled with CSF. (b) Sagittal CISS image along the long axis
of the cisternal segment of the right CN V (black arrow) shows the right superior cerebellar artery (white arrow) abutting the distal
cisternal segment of the nerve near the porus trigeminus without deformity in a patient with right TN. The Meckel’s cave (dashed arrow)
is seen particularly well on this image anterior to the porus trigeminus.
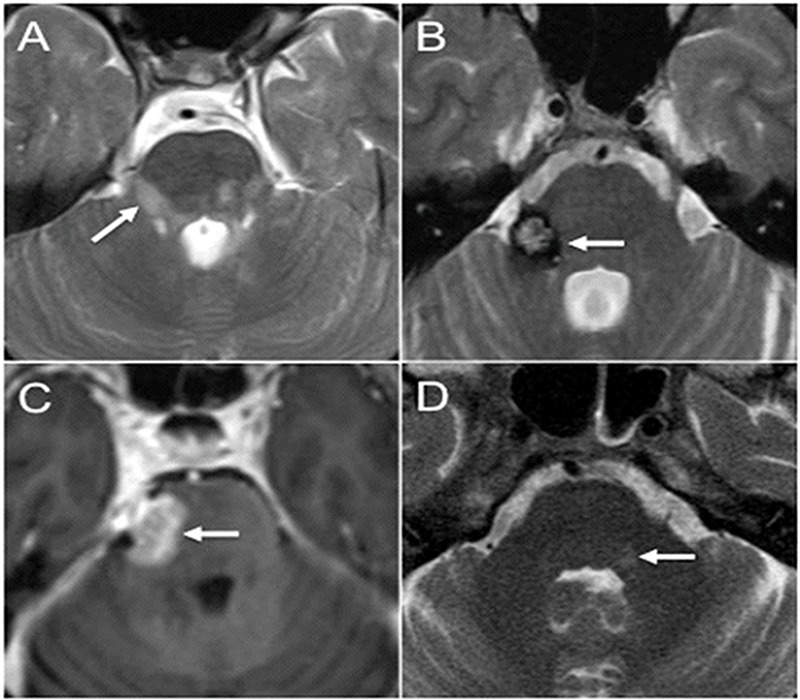
Brainstem lesions causing TN. (a) Axial T2-weighted image through the brainstem demonstrates multiple hyperintense lesions
in the posterior fossa in MS including a lesion extending along the expected course of the fascicular fibers and towards the root entry
zone of the right CN V (arrow). (b) Axial T2-weighted image through the brainstem shows a characteristic cavernous malformation
with central hyperintesities and surrounding hypointense hemosiderin rim (arrow). The lesion is centered in the right side of the pons
extending towards the root entry zone of the right CN V. The patient presented with right-sided TN. (c) Axial postcontrast T1-weighted
image shows abnormal enhancing lesion extending from the right side of the pons (arrow) into the cisternal segment of the right CN
V. Biopsy revealed primary CNS lymphoma. (d) Axial T2-weighted image through the pons shows asymmetric subtle hyperintense
signal along the cranial end of the trigeminal nucleus of CN V (arrow). The patient presented with left facial shingles and pain, and
was diagnosed with trigeminal zoster.
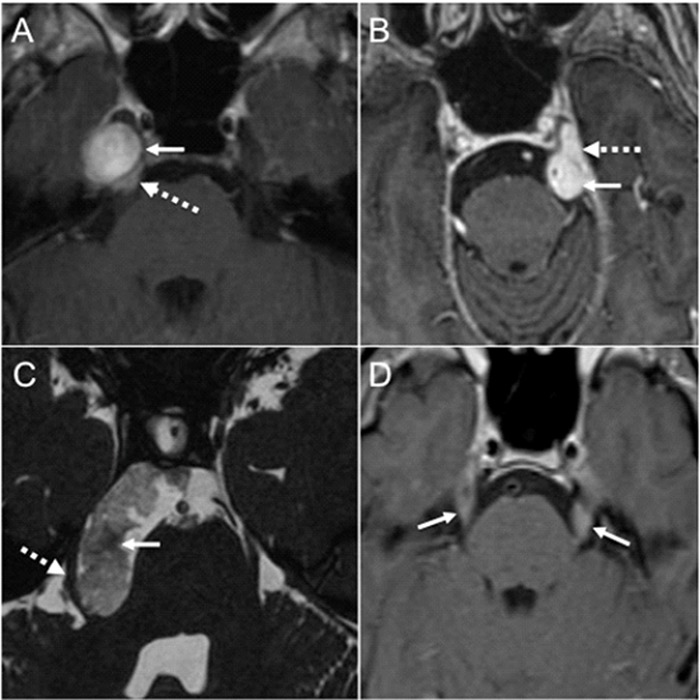
Lesions in the cisternal space and the Meckel’s cave causing TN. (a) Axial postcontrast T1-weighted image demonstrates a
round enhancing Schwannoma (arrow) centered in the right Meckel’s cave with mild posterior extension through the porus trigeminus
(dashed arrow). (b) Axial postcontrast T1-weighted image shows an avidly enhancing lesion in the left basal cisterns (arrow) with
anterior extension into the left Meckel’s cave (dashed arrow). The lesion was dural based arising from the dorsal left petroclival region,
a biopsy proven meningioma. It was deforming the cisternal segment of the left CN V. (c) Axial CISS image shows obvious deformity
of the cisternal segment of the right CN V (dashed arrow) caused by an epidermoid (arrow). The epidermoid demonstrated restricted
diffusion on diffusion weighted imaging (not shown). (d) Axial postcontrast T1-weighted image through the brainstem shows bilateral
smooth enhancement along the cisternal segment of CN V (arrows) in a patient with acute lymphoblastic leukemia. Additional cranial
nerve enhancement was present (not shown).
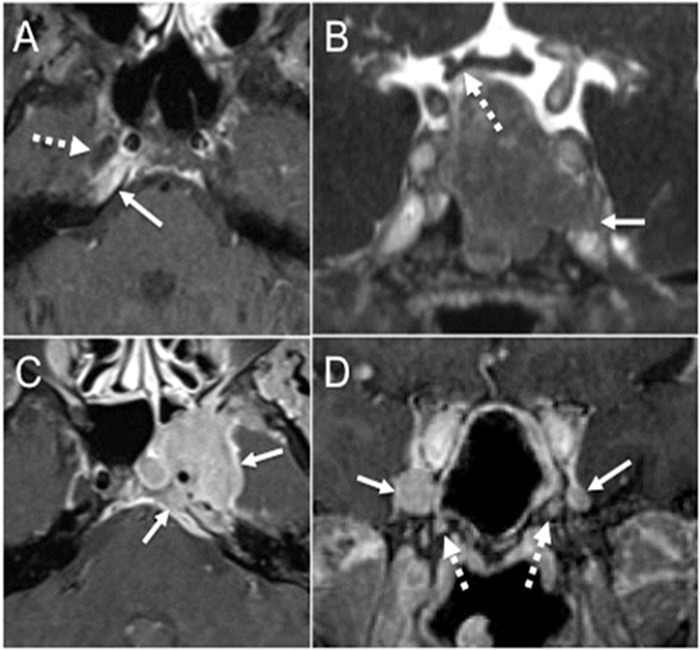
Skull base and cavernous sinus lesions. (a) Axial fat-suppressed post-contrast T1-weighted image shows asymmetric enhancement
in the right petrous apex (arrow) immediately posterior to the right Meckel’s cave (dashed arrow). This diabetic patient with petrous apicitis
presented with right facial pain and right abducens nerve palsy. (b) Coronal postcontrast CISS image through the pituitary gland shows a large
pituitary macroadenoma that infiltrates the left proximal cavernous sinus and the superior aspect of the left Meckel’s cave with effacement of
its normal fluid signal (arrow). The lesion superiorly abuts and mildly deforms the right side of the optic chiasm (dashed arrow). (c) Axial fatsuppressed
T1-weighted image shows a large enhancing mass (arrows) that infiltrates the left petroclival region, the left Meckel’s cave, and the
left cavernous sinus. This was a large nasopharyngeal carcinoma with contiguous intracranial extension. (d) Coronal postcontrast T1-weighted
image shows abnormal enlargement and enhancement of bilateral V2 in the anterior cavernous sinus worse on the right (arrows) due to perineural
spread from a large sinonasal adenoid cystic carcinoma. There is abnormal enhancement in bilateral vidian canals as well (dashed arrows).
References
-
- Yousry I, Moriggl B, Holtmannspoetter M, Schmid UD, Naidich TP, Yousry TA. Detailed anatomy of the motor and sensory roots of the trigeminal nerve and their neurovascular relationships: a magnetic resonance imaging study. J Neurosurg. 2004. September;101(3):427–34. 10.3171/jns.2004.101.3.0427 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources