

Acromioclavicular Joint Dislocation: Repair Through Open Ligament Transfer and Nonabsorbable Suture Fixation
- PMID: 29354426
- PMCID: PMC5622208
- DOI: 10.1016/j.eats.2017.05.004
Acromioclavicular Joint Dislocation: Repair Through Open Ligament Transfer and Nonabsorbable Suture Fixation
Abstract
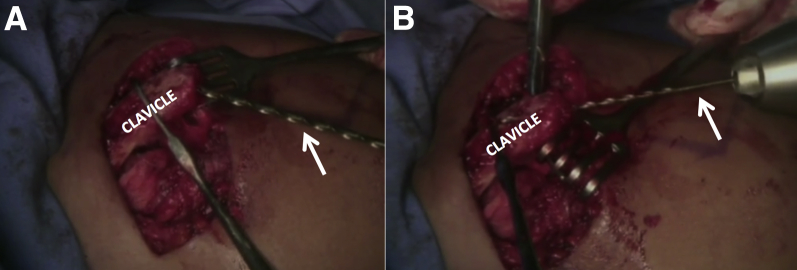
Acromioclavicular (AC) joint instability is a fairly common and particularly limiting injury that may result in persistent pain and reduced quality of life. In most cases, conservative management is successful. However, in the case of a severe AC joint dislocation, surgical intervention may be warranted. Previous surgical techniques for treatment of AC joint instability include screw fixation between the coracoid and clavicle, coracoacromial ligament transfer from its acromial insertion to the clavicle, and reconstruction of the coracoacromial and/or coracoclavicular ligaments. The purpose of this Technical Note is to describe our preferred technique for the treatment of a high-grade AC dislocation through coracoacromial ligament transfer to the lateral clavicle and nonabsorbable suture fixation between the coracoid process and clavicle.
Figures







References
-
- Pallis M., Cameron K.L., Svoboda S.J., Owens B.D. Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med. 2012;40:2072–2077. - PubMed
-
- Garretson R.B., III, Williams G.R., Jr. Clinical evaluation of injuries to the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003;22:239–254. - PubMed
-
- Ernberg L.A., Potter H.G. Radiographic evaluation of the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003;22:255–275. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
