

Circumferential Suture Repair of Isolated Horizontal Meniscal Tears Augmented With Fibrin Clot
- PMID: 29354475
- PMCID: PMC5709922
- DOI: 10.1016/j.eats.2017.06.031
Circumferential Suture Repair of Isolated Horizontal Meniscal Tears Augmented With Fibrin Clot
Abstract
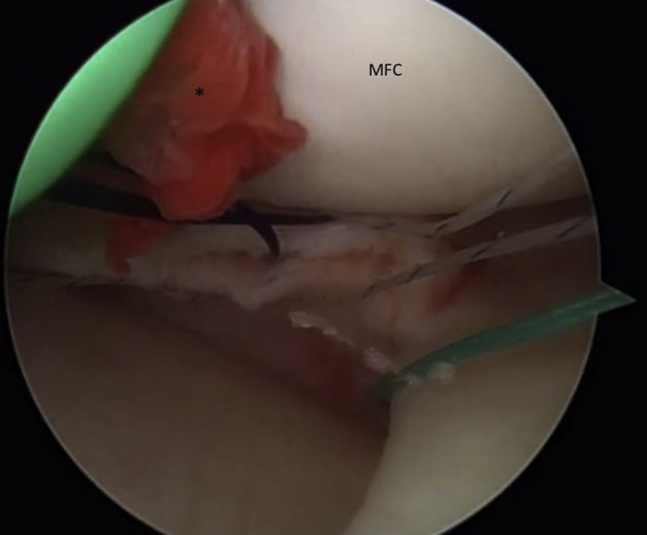
Traditionally, horizontal cleavage meniscus tears have been associated with osteoarthritis, indicative of the degenerative process. Recent treatment measures have focused on maintaining as much meniscal tissue as possible, despite the routine extension of these tears into the central white-white zones. In the absence of tunnel drilling for cruciate ligament reconstructions, the use of an exogenous fibrin clot is a useful adjunct to increase the local growth factors at the tear repair to aid in healing. This surgical technique is to describe the use of an all-arthroscopic tied circumferential suture repair of horizontal meniscal tears augmented with exogenous fibrin clot to treat all locations of horizontal meniscal tears.
Figures








References
-
- Voloshin A.S., Wosk J. Shock absorption of meniscectomized and painful knees: A comparative in vivo study. J Biomed Eng. 1983;5:157–161. - PubMed
-
- Cox J.S., Nye C.E., Schaefer W.W., Woodstein I.J. The degenerative effects of partial and total resection of the medial meniscus in dogs' knees. Clin Orthop Relat Res. 1975;109:178–183. - PubMed
-
- Newman A.P., Daniels A.U., Burks R.T. Principles and decision making in meniscal surgery. Arthroscopy. 1993;9:33–51. - PubMed
-
- Noble J., Hamblen D.L. The pathology of the degenerate meniscus lesion. J Bone Joint Surg Br. 1975;57:180–186. - PubMed
-
- Koh J.L., Yi S.J., Ren Y., Zimmerman T.A., Zhang L.Q. Tibiofemoral contact mechanics with horizontal cleavage tear and resection of the medial meniscus in the human knee. J Bone Joint Surg Am. 2016;98:1829–1836. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
